Halthcare


Archive for July 2016
Hepatitis a
Hepatitis A is a liver disease caused by the hepatitis A virus. The virus is primarily spread when an uninfected (and unvaccinated) person ingests food or water that is contaminated with the faeces of an infected person. The disease is closely associated with unsafe water or food, inadequate sanitation and poor personal hygiene.
Infectious agent
Hepatitis A virus (HAV) is the causative agent.
Symptoms
Illness due to hepatitis A typically causes acute fever, malaise, anorexia, nausea and abdominal discomfort. This is followed a few days later by dark urine and jaundice. Symptoms usually last several weeks although convalescence may sometimes be prolonged. Severe illness may rarely occur when hepatitis A infection complicates pre-existing liver disease. Infants and young children infected with HAV may have a mild
illness with few or no symptoms, with jaundice often being absent.
Method of diagnosis
A blood test indicating IgM anti-HAV antibodies confirms recent infection.These antibodies are present for two to
four months after infection. IgG antibodies alone are evidence of past
infection. In the acute stage of the illness, blood biochemistry shows elevated
transaminase levels indicating hepatocellular damage. The pattern of liver function tests may be non-specific
in later illness.
Incubation period
The incubation period is fifteen to fifty days, with an average of 28–30 days. Public health significance and occurrence Hepatitis A occurs worldwide. In developing countries most people are infected during childhood. With good sanitation and hygiene in the developed world, most people now reach adulthood without experiencing infection. There are about 70–200 cases per year in Victoria. Notifications have been declining nationally since the late 1990s. Infection is more common in travelers to endemic areas, injecting drug users, children in childcare and men who have sex with men. Common source outbreaks due to contaminated food are rare.
Reservoir
Humans.
Mode of transmission
Infection is transmitted by the faecal-oral route from person to person or via fomites. Infectious food handlers may
contaminate non-cooked foods such as salads. Infection can also occur through ingestion of contaminated food or water.Filter-feeding shellfish such as oysters raised in contaminated waters may harbour the virus.The precise timing and mode of transmission are often difficult to define.
Period of communicability
Cases are most infectious from the latter half of the incubation period until a few days after the onset of jaundice,corresponding to a peak in transaminase levels in cases without jaundice. Most
cases are not infectious after the first week of jaundice. Long term carriage or excretion of the virus does not occur.
Susceptibility and resistance
All non immune people are susceptible to infection. Immunity after infection is
probably lifelong. Control measures
Preventive measures
Education about good hygiene is important, particularly hand washing before handling food and eating and after
using the toilet. Inadequate sanitation and housing may contribute to endemic illness.Inactivated hepatitis A vaccines are available for use in persons two years of age and over. Protection begins within
14–21 days after the first dose. A second dose is required for long term protection.The vaccine is recommended for travellers to high risk areas, persons in high risk occupations such as childcare workers and emergency services personnel, injecting drug users and men who have sex with men.
Control of case
Treatment is generally supportive.Exclude from childcare, school or work for at least one week after the onset of
illness or jaundice and until they are well.Children must have a medical certificate
of recovery before returning to school or
child care.
Educate the patient and their family on the need for strict hygiene practices.
Infected persons should not prepare meals for others while infectious, nor share utensils, toothbrushes, towels and face washers.
Dispose of or thoroughly wash nappies of infants that have hepatitis A.
Control of contacts
Normal immunoglobulin (IG) 0.02 mL/kg body weight intramuscularly is recommended for:
• household and sexual contacts of the case
• staff and children in close contact with a case in a childcare centre.
IG is not recommended for usual office, school or factory contacts. IG must be given within seven to ten days of
exposure to be effective. IG is rarely given to persons exposed to a potential common source of hepatitis A such as food or water because cases related to such a source are usually recognised too long after the exposure for IG to be effective. Timely administration of IG will prevent or modify clinical illness for approximately six weeks after the dose. However, people exposed and infected before the administration of IG may still experience a mild infection, and may have the potential to infect others if strict personal hygiene is not maintained. Surveillance of contacts in a household or workplace should be maintained. Live vaccines such as Measles Mumps Rubella (MMR) should not be administered for three months after a dose of IG, and may also be ineffective if given in the 14 days prior to IG. Reschedule such routine vaccinations. When the case is a food handler:
• consider serological testing of coworkers to determine whether they have been infected or are susceptible
• place uninfected susceptible coworkers under surveillance and give them IG prophylaxis. These persons remain at a risk of developing mild illness modified by IG but can generally continue to work provided good personal hygiene and food handling practices are maintained
• undertake surveillance for hepatitis A in patrons by seeking a history of exposure to the food premises from
cases notified over the next two to three months
• carefully consider the role of the infected food handler. If transmission to patrons appears likely, consider urgent
follow-up of exposed patrons to offer them IG prophylaxis.Note that when the index case is a patron, it is usually
too late to offer IG prophylaxis to other diners, although personal contacts of the patron case should be offered IG
according to the usual protocol.When the case is a health care worker,the role of the case should be assessed
and consideration given to the provision of IG prophylaxis for co-workers and patients in their direct care whilst
infectious. Surveillance of contacts in the health care facility should be maintained.
Control of environment
A source of infection should always be sought. For apparently sporadic cases,consider contact with another known case and recent travel to an area where the disease is endemic. Acquisition of infection from young children, particularly those in childcare should be considered. Special attention should be given to toilet hygiene in schools and childcare centres. Ensure that soap and water are available and are used regularly to wash
hands.Food premises, health care facilities or child care centres where a case has worked whilst potentially infective should be requested to carry out a clean up in accordance with the Department’s Guidelines for the investigation of gastrointestinal illness.
Infectious agent
Hepatitis A virus (HAV) is the causative agent.
Symptoms
Illness due to hepatitis A typically causes acute fever, malaise, anorexia, nausea and abdominal discomfort. This is followed a few days later by dark urine and jaundice. Symptoms usually last several weeks although convalescence may sometimes be prolonged. Severe illness may rarely occur when hepatitis A infection complicates pre-existing liver disease. Infants and young children infected with HAV may have a mild
illness with few or no symptoms, with jaundice often being absent.
Method of diagnosis
A blood test indicating IgM anti-HAV antibodies confirms recent infection.These antibodies are present for two to
four months after infection. IgG antibodies alone are evidence of past
infection. In the acute stage of the illness, blood biochemistry shows elevated
transaminase levels indicating hepatocellular damage. The pattern of liver function tests may be non-specific
in later illness.
Incubation period
The incubation period is fifteen to fifty days, with an average of 28–30 days. Public health significance and occurrence Hepatitis A occurs worldwide. In developing countries most people are infected during childhood. With good sanitation and hygiene in the developed world, most people now reach adulthood without experiencing infection. There are about 70–200 cases per year in Victoria. Notifications have been declining nationally since the late 1990s. Infection is more common in travelers to endemic areas, injecting drug users, children in childcare and men who have sex with men. Common source outbreaks due to contaminated food are rare.
Reservoir
Humans.
Mode of transmission
Infection is transmitted by the faecal-oral route from person to person or via fomites. Infectious food handlers may
contaminate non-cooked foods such as salads. Infection can also occur through ingestion of contaminated food or water.Filter-feeding shellfish such as oysters raised in contaminated waters may harbour the virus.The precise timing and mode of transmission are often difficult to define.
Period of communicability
Cases are most infectious from the latter half of the incubation period until a few days after the onset of jaundice,corresponding to a peak in transaminase levels in cases without jaundice. Most
cases are not infectious after the first week of jaundice. Long term carriage or excretion of the virus does not occur.
Susceptibility and resistance
All non immune people are susceptible to infection. Immunity after infection is
probably lifelong. Control measures
Preventive measures
Education about good hygiene is important, particularly hand washing before handling food and eating and after
using the toilet. Inadequate sanitation and housing may contribute to endemic illness.Inactivated hepatitis A vaccines are available for use in persons two years of age and over. Protection begins within
14–21 days after the first dose. A second dose is required for long term protection.The vaccine is recommended for travellers to high risk areas, persons in high risk occupations such as childcare workers and emergency services personnel, injecting drug users and men who have sex with men.
Control of case
Treatment is generally supportive.Exclude from childcare, school or work for at least one week after the onset of
illness or jaundice and until they are well.Children must have a medical certificate
of recovery before returning to school or
child care.
Educate the patient and their family on the need for strict hygiene practices.
Infected persons should not prepare meals for others while infectious, nor share utensils, toothbrushes, towels and face washers.
Dispose of or thoroughly wash nappies of infants that have hepatitis A.
Control of contacts
Normal immunoglobulin (IG) 0.02 mL/kg body weight intramuscularly is recommended for:
• household and sexual contacts of the case
• staff and children in close contact with a case in a childcare centre.
IG is not recommended for usual office, school or factory contacts. IG must be given within seven to ten days of
exposure to be effective. IG is rarely given to persons exposed to a potential common source of hepatitis A such as food or water because cases related to such a source are usually recognised too long after the exposure for IG to be effective. Timely administration of IG will prevent or modify clinical illness for approximately six weeks after the dose. However, people exposed and infected before the administration of IG may still experience a mild infection, and may have the potential to infect others if strict personal hygiene is not maintained. Surveillance of contacts in a household or workplace should be maintained. Live vaccines such as Measles Mumps Rubella (MMR) should not be administered for three months after a dose of IG, and may also be ineffective if given in the 14 days prior to IG. Reschedule such routine vaccinations. When the case is a food handler:
• consider serological testing of coworkers to determine whether they have been infected or are susceptible
• place uninfected susceptible coworkers under surveillance and give them IG prophylaxis. These persons remain at a risk of developing mild illness modified by IG but can generally continue to work provided good personal hygiene and food handling practices are maintained
• undertake surveillance for hepatitis A in patrons by seeking a history of exposure to the food premises from
cases notified over the next two to three months
• carefully consider the role of the infected food handler. If transmission to patrons appears likely, consider urgent
follow-up of exposed patrons to offer them IG prophylaxis.Note that when the index case is a patron, it is usually
too late to offer IG prophylaxis to other diners, although personal contacts of the patron case should be offered IG
according to the usual protocol.When the case is a health care worker,the role of the case should be assessed
and consideration given to the provision of IG prophylaxis for co-workers and patients in their direct care whilst
infectious. Surveillance of contacts in the health care facility should be maintained.
Control of environment
A source of infection should always be sought. For apparently sporadic cases,consider contact with another known case and recent travel to an area where the disease is endemic. Acquisition of infection from young children, particularly those in childcare should be considered. Special attention should be given to toilet hygiene in schools and childcare centres. Ensure that soap and water are available and are used regularly to wash
hands.Food premises, health care facilities or child care centres where a case has worked whilst potentially infective should be requested to carry out a clean up in accordance with the Department’s Guidelines for the investigation of gastrointestinal illness.
Treatment
There is no specific treatment for hepatitis A. Recovery from symptoms following infection may be slow and may take several weeks or months. Most important is the avoidance of unnecessary medications. Acetaminophen / Paracetamol and medication against vomiting should not be given.Hospitalization is unnecessary in the absence of acute liver failure. Therapy is aimed at maintaining comfort and adequate nutritional balance, including replacement of fluids that are lost from vomiting and diarrhoea.
Infectious Diarrhea. Causes,symptoms,Diarrhea treatment.
Diarrhea. An increased frequency of defecation due to a microbial pathogen and defined as greater than 3 stools per day or greater than 200 g of stool per day.
B. Epidemiology
1. Infectious diarrhea is the most common cause of diarrhea worldwide.
2. The second most common cause of death worldwide but the leading cause of childhood death worldwide.
3. In the United States, most episodes occur during the winter months and are due to viral pathogens (eg, noroviruses, rotaviruses).
C. D iarrhea Syndromes
1. Acute infectious diarrhea. Lasting less than 14 days.
a. Acute watery diarrhea without blood
b. Acute dysentery (diarrhea with blood)
2. Chronic or persistent diarrhea. Lasting more than 14 days.
D. Pathogenesis. Pathogens are transmitted through contaminated water or foods/food products and reach the gastrointestinal tract to cause:
1. Increased intestinal secretion of fluid and electrolytes, most commonly in the small intestine, through the production of enterotoxins (eg,cholera toxin, Escherichia coli heat labile and heat stable toxins) that may mediate secretagogues (eg, 5-hydroxytryptamine [5-HT]).
2. Decreased intestinal absorption of fluid and electrolytes in the small and large intestine through intestinal mucosal damage. Severe villous atrophy can occur with infection due to Giardia, Cryptosporidium, Cyclospora, and Microsporidium (intestinal protozoa). An alternative cause of villous atrophy is celiac disease (an autoimmune disorder due to gluten intolerance).
CAUSES OF INFECTIOUS DIARRHEA.
A. Bacterial1. Campylobacter jejuni. Most commonly from a foodborne exposure to
poultry.
2. Salmonella spp
a. Nontyphoid. Most commonly from a foodborne exposure to poultry or eggs.
b. Typhoid and paratyphoid. Person-to-person contact during international travel.
3. Shigella spp. Person-to-person contact.
4. Shiga toxin–E coli (0157:H7). Most commonly a foodborne exposure to undercooked beef or raw seed sprouts.
5. Vibrio spp
a. Cholera. Low level of endemicity in U.S. Gulf Coast states with transmission by water exposure or seafood exposure.
b. Noncholera. Most commonly foodborne exposure to shellfish and seafood.
6. Yersinia enterocolitica. Can be associated with swine and cattle exposure.
7. Aeromonas spp. International travel to tropical regions.
8. Plesiomonas shigelloides. International travel and ingestion of seafood.
9. Staphylococcus aureus. Foodborne exposure (eg, potato salad) due to preformed toxin.
10. Clostridium perfringens. Contaminated meat, vegetables, or poultry
with bacterial spores.
11. Bacillus cereus. Contaminated rice (reheated rice) and vegetable sprouts with bacterial spores.
12. Clostridium difficile.
B. Viruses. Most commonly occur during the winter months and are typically due to outbreaks in families, nursing homes, or day care centers (usually selflimiting
and less than one day).
1. Noroviruses.
2. Rotavirus.
3. Enteric adenoviruses (types 40 and 41).
4. Cytomegalovirus (CMV). More common in immunocompromised patients.
C. Parasites. Most commonly related to international travel and/or contaminated
water. Diarrhea usually persists for greater than 7 to 10 days.
1. Giardia intestinalis
2. Cryptosporidium parvum
3. Cyclospora cayetanensis
4. Microsporidia spp
5. Entameba histolytica. (Africa, Asia, Latin America).
6. Balantidium coli. (Asia).
Clinical Manifes tations of Infectious Diarrhea(SYMPTOMS).
A. D iarrhea. Usually one of two forms, but there can be considerable overlap.
1. Watery diarrhea without blood. Usually self-limiting and clinically nonspecific to etiology.
2. Diarrhea with blood (dysentery). Usually indicates colitis (ie, inflammatory diarrhea). Associated with fever, nausea, and abdominal pain and cramps. Most commonly due to Shigella, Campylobacter, nontyphoid Salmonella, and Shiga toxin–E coli. Also, can be associated with Aeromonas spp, Yersinia spp, noncholeraic Vibrio, and E histolytica.
B. Abdominal Pain and Cramps. Usually associated with dysentery but can also occur without dysentery.

C. N ausea and Vomiting. May be associated with abdominal pain and cramps but is typically due to viral illnesses.
D. F ever. Usually occurs with acute dysentery (ie, inflammatory diarrhea) or bacteremia from salmonella.
E. T enesmus. May indicate inflammatory diarrhea and is characterized as a feeling of a constant need to defecate.
F. D elirium or Altered Mental Status. Usually indicates dehydration and is usually associated with other findings such as tachycardia, dry mucous membranes,and poor skin turgor.
Approach to the Patient.A. H istory. A complete history should be performed with attention to exposures or risk factors associated with infectious diarrhea, comorbid illnesses
(immunocompromised or pregnant patients may be at risk for certain infections), medications, recent travel history, and occupation (eg, day care or nursing home worker). Additionally, diarrhea in family members and the timing of diarrhea onset may be helpful:
1. Incubation period less than 6 hours. (S aureus or B cereus.)
2. Incubation period 6 to 24 hours. (C perfringens or B cereus.)
3. Incubation period 16 to 72 hours. (All other causes.)
B. Physical Examination. A complete physical examination should be performed
with focused attention on:
1. Neurologic examination (to assess mental status by the Glasgow coma cale).
2. HEENT examination (dry mucous membranes can suggest dehydration).
3. Cardiovascular examination (resting tachycardia or orthostatic hypotension may suggest dehydration).
4. Musculoskeletal examination (joint pain may suggest Yersinia spp or
C jejuni as Reiter syndrome).
5. Rectal examination (to detect blood in the stool that may indicate dysentery).
Because the most feared complication of infectious diarrhea is dehydration, the clinical evaluation of the degree of dehydration remains important. (The followingare general considerations that would vary among different patients.)
1. Mild-to-Moderate Dehydration (3% to 9% Fluid Loss)
a. Fatigue and restlessness
b. Dry mucous membranes and thirst sensation
c. Weak pulses and cool extremities
d. Decreased urine output (may be indicated by a dark-concentrated urine and with less than 800 mL per day)
2. Severe Dehydration (Greater than 10% Fluid Loss)
a. Apathy and lethargy
b. Dry mucous membranes, sunken eyes, and extreme thirst sensation
c. Deep breaths and tachycardia
d. Skin tenting, poor capillary refill, weak pulses, and cool extremities
e. Minimal urine output (less than 500 mL dark-concentrated urine per day)
C. Laboratory Studies
1. CBC(COMPLETE BLOOD COUNT). Nonspecific. An elevated hematocrit may suggest dehydration.
2. BMP. Infectious diarrhea may produce a non–gap metabolic acidosis in association with electrolyte abnormalities (eg, hypernatremia, hypokalemia). An elevated BUN, creatinine, and metabolic alkalosis may suggest dehydration.
3. Blood cultures. Usually not ordered and of low yield; however, bacteremia may occur with Salmonella spp–related infections.
4. Stool leukocytes and/or lactoferrin. May be helpful for inflammatory diarrhea, but nonspecific.
a. Stool leukocytes. Sensitivity 73% and specificity 84% for bacterial infectious diarrhea. A small content of stool mucus or liquid stool is stained with methylene blue stain or Wright stain and then examined for leukocytes. A false-negative test may occur with cytotoxogenic
C difficile or E histolytica infection due to destruction of leukocytes.
b. Stool lactoferrin. Sensitivity 92% and specificity 79% for bacterial infectious diarrhea. Lactoferrin is a glycoprotein found in neutrophil granules and is detected by a rapid immunologic latex agglutination method. The test performance is not altered by the destruction of
leukocytes.
5. Stool cultures. The diagnostic yield is estimated from 1% to 5%. Indicated when patients have any of the following:
a. Severe diarrhea (greater than 6 stools per day)
b. Dysentery
c. Diarrhea associated with fever
d. Persistent diarrhea (over more than 7 days)
e. Multiple cases of diarrhea
TREATMENT
A. Supportive Care. Should be provided in all cases and can consist of fluid and electrolyte replacement, a diet of easily digestible foods (eg, BRAT diet: bananas, rice, applesauce, and toast), and/or antimotility medications (eg, loperamide). Antimotility medications should be avoided in patients with dysentery or suspected inflammatory diarrhea. Patients should avoid milk or other dairy products due to the development of transient lactose intolerance.
B. Oral Rehydration Therapy. The initial treatment of infectious diarrhea should focus on the prevention of dehydration with rehydration efforts. Commercialformulations (eg, Pedialyte) can be obtained and used according to the listed directions; however, as a general rule, a homemade oral rehydration solution can be produced by the following formula: add 1 tablespoon of salt and
2 tablespoons of sugar to 1 liter of water.Treatment recommendations according to the degree of dehydration include the following. (These are general rules to the approach to rehydration
and may not apply to all patients.)
1. Minimal Dehydration (Less than 3% Fluid Loss)
a. Less than 10 kg weight: 60–120 mL of oral rehydration solution per diarrhea stool
b. Greater than 10 kg weight: 120–240 mL of oral rehydration solution per diarrhea stool
2. Mild-to-Moderate Dehydration (3% to 9% Fluid Loss)
a. May be treated as an outpatient
b. 50–100 mL per kg of body weight replaced over a 3- to 4-hour period of time
B. Epidemiology
1. Infectious diarrhea is the most common cause of diarrhea worldwide.
2. The second most common cause of death worldwide but the leading cause of childhood death worldwide.
3. In the United States, most episodes occur during the winter months and are due to viral pathogens (eg, noroviruses, rotaviruses).
C. D iarrhea Syndromes
1. Acute infectious diarrhea. Lasting less than 14 days.
a. Acute watery diarrhea without blood
b. Acute dysentery (diarrhea with blood)
2. Chronic or persistent diarrhea. Lasting more than 14 days.
D. Pathogenesis. Pathogens are transmitted through contaminated water or foods/food products and reach the gastrointestinal tract to cause:
1. Increased intestinal secretion of fluid and electrolytes, most commonly in the small intestine, through the production of enterotoxins (eg,cholera toxin, Escherichia coli heat labile and heat stable toxins) that may mediate secretagogues (eg, 5-hydroxytryptamine [5-HT]).
2. Decreased intestinal absorption of fluid and electrolytes in the small and large intestine through intestinal mucosal damage. Severe villous atrophy can occur with infection due to Giardia, Cryptosporidium, Cyclospora, and Microsporidium (intestinal protozoa). An alternative cause of villous atrophy is celiac disease (an autoimmune disorder due to gluten intolerance).
CAUSES OF INFECTIOUS DIARRHEA.
A. Bacterial1. Campylobacter jejuni. Most commonly from a foodborne exposure to
poultry.
2. Salmonella spp
a. Nontyphoid. Most commonly from a foodborne exposure to poultry or eggs.
b. Typhoid and paratyphoid. Person-to-person contact during international travel.
3. Shigella spp. Person-to-person contact.
4. Shiga toxin–E coli (0157:H7). Most commonly a foodborne exposure to undercooked beef or raw seed sprouts.
5. Vibrio spp
a. Cholera. Low level of endemicity in U.S. Gulf Coast states with transmission by water exposure or seafood exposure.
b. Noncholera. Most commonly foodborne exposure to shellfish and seafood.
6. Yersinia enterocolitica. Can be associated with swine and cattle exposure.
7. Aeromonas spp. International travel to tropical regions.
8. Plesiomonas shigelloides. International travel and ingestion of seafood.
9. Staphylococcus aureus. Foodborne exposure (eg, potato salad) due to preformed toxin.
10. Clostridium perfringens. Contaminated meat, vegetables, or poultry
with bacterial spores.
11. Bacillus cereus. Contaminated rice (reheated rice) and vegetable sprouts with bacterial spores.
12. Clostridium difficile.
B. Viruses. Most commonly occur during the winter months and are typically due to outbreaks in families, nursing homes, or day care centers (usually selflimiting
and less than one day).
1. Noroviruses.
2. Rotavirus.
3. Enteric adenoviruses (types 40 and 41).
4. Cytomegalovirus (CMV). More common in immunocompromised patients.
C. Parasites. Most commonly related to international travel and/or contaminated
water. Diarrhea usually persists for greater than 7 to 10 days.
1. Giardia intestinalis
2. Cryptosporidium parvum
3. Cyclospora cayetanensis
4. Microsporidia spp
5. Entameba histolytica. (Africa, Asia, Latin America).
6. Balantidium coli. (Asia).
Clinical Manifes tations of Infectious Diarrhea(SYMPTOMS).
A. D iarrhea. Usually one of two forms, but there can be considerable overlap.
1. Watery diarrhea without blood. Usually self-limiting and clinically nonspecific to etiology.
2. Diarrhea with blood (dysentery). Usually indicates colitis (ie, inflammatory diarrhea). Associated with fever, nausea, and abdominal pain and cramps. Most commonly due to Shigella, Campylobacter, nontyphoid Salmonella, and Shiga toxin–E coli. Also, can be associated with Aeromonas spp, Yersinia spp, noncholeraic Vibrio, and E histolytica.
B. Abdominal Pain and Cramps. Usually associated with dysentery but can also occur without dysentery.

C. N ausea and Vomiting. May be associated with abdominal pain and cramps but is typically due to viral illnesses.
D. F ever. Usually occurs with acute dysentery (ie, inflammatory diarrhea) or bacteremia from salmonella.
E. T enesmus. May indicate inflammatory diarrhea and is characterized as a feeling of a constant need to defecate.
F. D elirium or Altered Mental Status. Usually indicates dehydration and is usually associated with other findings such as tachycardia, dry mucous membranes,and poor skin turgor.
Approach to the Patient.A. H istory. A complete history should be performed with attention to exposures or risk factors associated with infectious diarrhea, comorbid illnesses
(immunocompromised or pregnant patients may be at risk for certain infections), medications, recent travel history, and occupation (eg, day care or nursing home worker). Additionally, diarrhea in family members and the timing of diarrhea onset may be helpful:
1. Incubation period less than 6 hours. (S aureus or B cereus.)
2. Incubation period 6 to 24 hours. (C perfringens or B cereus.)
3. Incubation period 16 to 72 hours. (All other causes.)
B. Physical Examination. A complete physical examination should be performed
with focused attention on:
1. Neurologic examination (to assess mental status by the Glasgow coma cale).
2. HEENT examination (dry mucous membranes can suggest dehydration).
3. Cardiovascular examination (resting tachycardia or orthostatic hypotension may suggest dehydration).
4. Musculoskeletal examination (joint pain may suggest Yersinia spp or
C jejuni as Reiter syndrome).
5. Rectal examination (to detect blood in the stool that may indicate dysentery).
Because the most feared complication of infectious diarrhea is dehydration, the clinical evaluation of the degree of dehydration remains important. (The followingare general considerations that would vary among different patients.)
1. Mild-to-Moderate Dehydration (3% to 9% Fluid Loss)
a. Fatigue and restlessness
b. Dry mucous membranes and thirst sensation
c. Weak pulses and cool extremities
d. Decreased urine output (may be indicated by a dark-concentrated urine and with less than 800 mL per day)
2. Severe Dehydration (Greater than 10% Fluid Loss)
a. Apathy and lethargy
b. Dry mucous membranes, sunken eyes, and extreme thirst sensation
c. Deep breaths and tachycardia
d. Skin tenting, poor capillary refill, weak pulses, and cool extremities
e. Minimal urine output (less than 500 mL dark-concentrated urine per day)
C. Laboratory Studies
1. CBC(COMPLETE BLOOD COUNT). Nonspecific. An elevated hematocrit may suggest dehydration.
2. BMP. Infectious diarrhea may produce a non–gap metabolic acidosis in association with electrolyte abnormalities (eg, hypernatremia, hypokalemia). An elevated BUN, creatinine, and metabolic alkalosis may suggest dehydration.
3. Blood cultures. Usually not ordered and of low yield; however, bacteremia may occur with Salmonella spp–related infections.
4. Stool leukocytes and/or lactoferrin. May be helpful for inflammatory diarrhea, but nonspecific.
a. Stool leukocytes. Sensitivity 73% and specificity 84% for bacterial infectious diarrhea. A small content of stool mucus or liquid stool is stained with methylene blue stain or Wright stain and then examined for leukocytes. A false-negative test may occur with cytotoxogenic
C difficile or E histolytica infection due to destruction of leukocytes.
b. Stool lactoferrin. Sensitivity 92% and specificity 79% for bacterial infectious diarrhea. Lactoferrin is a glycoprotein found in neutrophil granules and is detected by a rapid immunologic latex agglutination method. The test performance is not altered by the destruction of
leukocytes.
5. Stool cultures. The diagnostic yield is estimated from 1% to 5%. Indicated when patients have any of the following:
a. Severe diarrhea (greater than 6 stools per day)
b. Dysentery
c. Diarrhea associated with fever
d. Persistent diarrhea (over more than 7 days)
e. Multiple cases of diarrhea
TREATMENT
A. Supportive Care. Should be provided in all cases and can consist of fluid and electrolyte replacement, a diet of easily digestible foods (eg, BRAT diet: bananas, rice, applesauce, and toast), and/or antimotility medications (eg, loperamide). Antimotility medications should be avoided in patients with dysentery or suspected inflammatory diarrhea. Patients should avoid milk or other dairy products due to the development of transient lactose intolerance.
B. Oral Rehydration Therapy. The initial treatment of infectious diarrhea should focus on the prevention of dehydration with rehydration efforts. Commercialformulations (eg, Pedialyte) can be obtained and used according to the listed directions; however, as a general rule, a homemade oral rehydration solution can be produced by the following formula: add 1 tablespoon of salt and
2 tablespoons of sugar to 1 liter of water.Treatment recommendations according to the degree of dehydration include the following. (These are general rules to the approach to rehydration
and may not apply to all patients.)
1. Minimal Dehydration (Less than 3% Fluid Loss)
a. Less than 10 kg weight: 60–120 mL of oral rehydration solution per diarrhea stool
b. Greater than 10 kg weight: 120–240 mL of oral rehydration solution per diarrhea stool
2. Mild-to-Moderate Dehydration (3% to 9% Fluid Loss)
a. May be treated as an outpatient
b. 50–100 mL per kg of body weight replaced over a 3- to 4-hour period of time
Fever of Unknown Origin.Causes,signs,symptoms,treatment.
I. Introduction.A. C lassic Fever of Unknown Origin (FUO ) Definition. A temperature record on
multiple occasions that is greater than 38.3°C (101°F) for more than 3-weeks’ duration despite 1 week of logical diagnostic evaluation in the hospital.
B. R evised Classic FUO Definitions and Further Classifications. A fever lasting more than 3 weeks with recordings greater than 38.3°C (101°F) despite logical diagnostic evaluation during 3 days in the hospital or 3 outpatient clinic evaluations.
1. Classic FUO. Defined above with the most common etiologies within 3 main categories: infection, malignancy, or collagen-vascular disease.
2. Nosocomial FUO. Usually a fever occurring in a patient that has been hospitalized for at least 24 hours without a defined source prior to admission or 3 days of evaluation. The more common etiologies of a nosocomial fever include urinary tract infections, catheter-related infections, pneumonia,Clostridium difficile colitis, pulmonary embolism, DVT, septic thrombophlebitis,
gastrointestinal bleed, or medication-induced fever.
3. Neutropenia FUO. A recurrent or persistent fever in a patient with neutropenia (absolute neutrophil count less than 500 cells/mm³ or 0.5 3 109/L] despite 3 days of logical diagnostic evaluation. The more common etiologies include nosocomial etiologies (as above) as well as opportunistic bacterial infections (see below), aspergillosis, candidiasis (eg, hepatosplenic
candidiasis), or HSV/VZV.
4. HIV-related FUO. A recurrent or persistent fever for greater than 4 weeks in a patient seropositive for HIV despite 3 days of logical diagnostic evaluation in the hospital. The more common etiologies include: Mycobacterium avium-intracellulare complex (MAC), CMV, Pneumocystis jiroveci p., lymphoma, Kaposi sarcoma, toxoplasmosis, cryptococcus, or medications.

II. Ca uses of FUO .While greater than 200 possible causes for FUO have been reported, the following lists are the more common causes to be considered initially.A cause may not be found in as many as 20% to 30% of cases. The causes are listed by the three main etiologic categories:
A. Infection. This group of causes has been estimated to occur in 28% of FUO cases. The etiologies to initially consider include:
1. Tuberculosis (Mycobacterium tuberculosis; pulmonary and extrapulmonary disease.
2. Abdominal or pelvic abscess (most common cause in the elderly age group).
3. Sinusitis (most commonly with chronic infections or hospitalized patients with nasogastric tubes).
4. Dental abscess (usually oral bacterial flora and may or may not be associated with a recent dental procedure).
5. Endocarditis (most commonly culture negative endocarditis).
6. Osteomyelitis (most commonly chronic osteomyelitis).
7. Hepatitis or chronic biliary tract infections
8. Prostatitis (especially with a recent prostate procedure and is characterized by chronic pelvic pain).
9. HIV infection or sexually transmitted disease
10. CMV (cytomegalovirus; especially in immunocompromised patients).
11. EBV (Epstein-Barr virus; especially following posthematopoietic stem cell transplantation).
12. HSV or VZV (herpes simplex virus and varicella-zoster virus; most commonly associated with reactivation infections in immunocompromised patients).
13. Rocky Mountain spotted fever or Lyme disease (Rickettsia rickettsii or Borrelia burgdorferi; usually associated with outdoor activities and a tick bite).
14. Q fever (Coxiella burnetii; associated with exposure to farm animals [cattle, sheep, or goats] and is characterized by flu-like symptoms with fevers, pneumonia, and hepatitis).
15. Brucellosis (Brucella spp; associated with exposure to animals [goats, sheep, bison, or swine] and is characterized by intermittent fevers, gastrointestinal symptoms [eg, nausea, abdominal pain], and joint effusions).
16. Leptospirosis (Leptospira interrogans; usually associated with rodents or colonized dogs [the organism resides in the renal tubules and is shed in the urine] during recreational activities and is characterized by malaise, headaches, myalgias, abdominal pain, and conjunctival
erythema).
17. Psittacosis (Chlamydophila psittaci; usually associated with birds, especially parrots, and is characterized by fevers, chills, malaise, myalgias, and nonproductive cough).
18. Malaria (Plasmodium spp; transmitted by the Anopheles mosquito and usually characterized by periodic fevers, chills, and rigors).
19. Leishmaniasis (a group of obligate intracellular parasites that are transmitted by sand flies [genera Phlebotomus and Lutzomyia]; commonly associated with cutaneous lesions [eg, a necrotic ulcer] but can be associated with fevers, chills, diarrhea, weight loss, and hepatosplenomegaly).
20. Babesiosis (Babesia spp; an intraerythrocyte parasitic infection transmitted by the bite of an Ixodes tick and characterized by fevers, chills,night sweats, fatigue, weakness, and anemia).
21. Enteric fever (Salmonella enterica, serovar Typhi; associated with travel and characterized by fevers, headaches, myalgias, malaise, and gastrointestinal pain).
22. Toxoplasmosis (Toxoplasma gondii; most commonly a reactivation infection in immunocompromised patients).
23. Rat-bite fever (Streptobacillus moniliformis; patients have an exposure to rats and the disorder is characterized by fevers, headaches, chills, polyarthralgias, and a maculopapular rash on the hands and/or feet).
24. Catscratch disease (Bartonella henselae; a disorder characterized by fevers and localized adenopathy with an exposure to cats).
25. Whipple disease (Tropheryma whippelii; a disorder characterized by
fevers, arthralgia, abdominal pain, chronic diarrhea, weight loss, and generalized lymphadenopathy).
26. Mycobacterium avium-intracellulare complex (MAC; usually associated with fevers and cavitary pulmonary disease in immunocompromised patients).
27. Pneumocystis jirovecii pneumonia (almost exclusively associated with acute hypoxic pneumonia in immunocompromised patients, especially acquired immune deficiency syndrome patients with a CD4 cell count below 200 cells/mm3).
28. Cryptococcus neoformans (commonly associated with chronic corticosteroid use or immunocompromised patients and usually presents as fevers with meningitis or pulmonary pneumonia).
29. Aspergillosis (Aspergillus spp; opportunistic pathogens that can be associated with fevers and pulmonary cavities or endocarditis).
30. Candidiasis (Candida spp; opportunistic pathogens that can be associated with fevers and catheter infections, endocarditis, or hepatosplenic candidiasis).
B. Malignancy. This group typically accounts for 17% of cases. The etiologies to
initially consider include:
1. Leukemia (more commonly chronic leukemia).
2. Lymphoma (most common cause in this group—Hodgkin and non- Hodgkin lymphoma).
3. Renal cell carcinoma.
4. Colorectal cancers.
5. Myelodysplastic syndrome.
6. Pancreatic carcinoma (most commonly not associated with biliary or pancreatic duct obstruction).
7. Metastatic cancer with or without known primary.
C. C ollagen Vascular Disease. This group is estimated to account for 21% of
cases. The etiologies to initially consider include:
1. Temporal arteritis (more common over the age of 50).
2. Rheumatoid arthritis.
3. SLE.
4. Polymyalgia rheumatic.
5. Vasculitis.
6. Polychondritis.
7. Polymyositis.
8. Adult Still disease or adult juvenile rheumatoid arthritis.
9. Sjögren syndrome or Behçet syndrome.
D. Miscellaneous. This group accounts for 5% to 10% of cases. The etiologies
to initially consider include:
1. Crohn disease or ulcerative colitis.
2. Thyroiditis.
3. Sarcoidosis.
4. Amyloidosis.
5. Gout or pseudogout.
6. Addison disease.
7. Hemochromatosis.
8. Medications. The fever usually resolves within 2 to 5 days of discontinuation of the medication. More common medications to consider include:
a. Antibiotics (penicillin, cephalosporin, sulfonamide, tetracycline, and rifampin)
b. Anticonvulsants (phenytoin, carbamazepine, and barbiturates)
c. Antihistamines
d. Nonsteroidal anti-inflammatory drugs (NSAIDs)
e. Iodine and iodide agents (eg, contrast dye)
III. C linical Manif estations of FUO . While documentation of fever is required to establish the diagnosis of FUO, there is no significant relationship between the fever pattern and underlying etiology. However, some associations have been suggested:
A. D ouble Quotidian Fever. Defined as a fever with two peaks within 24 hours;
conditions to consider include endocarditis, malaria, military Mycobacterium
tuberculosis, adult Still disease, and leishmaniasis.
B. S ustained Fever. Defined as a continuously elevated temperature and most
commonly associated with CNS injury (eg, stroke, bleed, etc) or pneumonia
(most commonly secondary to a gram-positive pathogen).
C. Pel-Ebstein Fever. A daily fever that resolves only to reoccur again with a
similar pattern; consider Hodgkin disease.
D. Periodic or Relapsing Fever. Consider endocarditis, malaria, lymphoma, Lyme disease, RMSF, or rat-bite fever.
E. E arly Morning Fever Spike. Consider Mycobacterium tuberculosis, polyarteritis nodosa, brucellosis, or salmonellosis. In general, there are no classic symptoms or signs pathognomonic for a particular FUO etiology, and conditions or causes may be a typical or atypical presentation for a particular disease. It should also be emphasized that no symptom or sign be regarded as irrelevant in a patient suspected of FUO.
IV. App roach to the Patient with FUO
A. H istory. The most important initial approach to the patient with FUO is documenting the fever and recording a complete, accurate, and comprehensive history. Physicians must be meticulous and systematic when obtaining information for the following key elements:
1. Age. Certain illnesses may be more likely associated with particular age groups (eg, malignancy, temporal arteritis, and intra-abdominal abscess may be more likely in persons over the age of 50).
2. History of present illness. While most patients exhibit atypical manifestation, it is important to establish in chronological fashion the onset of symptoms and events that may be related to the fever.
3. Past medical history. This area should focus on any recent or chronic medical illness or infection; and any prior diagnosis of malignancy; and any prior surgery or complication related to surgery; and any implanted prosthetic device, prosthetic valve, pacemaker or implantable defibrillator,
cosmetic implanted surgical device, indwelling venous catheter, or implanted vascular graft.
4. Medications. A complete list of prescription, over-the-counter, and herbal medications should be documented. Drug-related fevers are more common in the elderly and HIV seropositive patient groups.
5. Allergies. Medication allergies may suggest a drug fever while environmental allergies may suggest an atopic condition.
6. Social history. This should include information about the patient’s country of origin, immigration status, prior country or state of residence, travel history (with relevant exposure, vaccination, and prophylaxis history), vaccination status, occupation and occupational risks, smoking status,alcohol and drug exposure, hobbies or leisure activities, pet or animal exposure, dietary (usual or unusual) habits, and sexual activity.
7. Family history. It is important to establish any recent or prior illness in family members and any unusual hereditary cause for fever (eg, familial Mediterranean fever).
B. Physical Examination. A complete physical examination should be performed with attention to all body systems. While physicians should be meticulous and conduct the examination in a systematic approach, repeat examinations are often helpful as diagnostic clues may be either atypical or obscure for the cause of the FUO. Areas of the physical examination that require careful attention and common associations include:
1. Dermatologic examination.
a. Rose spot (typhoid or psittacosis)
b. Hyperpigmentation (hemochromatosis, Addison disease, or Whipple disease)
c. Petechial rash (RMSF)
d. Erythema multiforme (Lyme disease)
e. Vesicular rash on an erythematous base (HSV or VZV)
2. Cardiovascular examination. A new diastolic murmur or change with existing murmur may suggest endocarditis or atrial myxoma.
3. Oral-pharyngeal examination.
a. Gingivitis and/or poor dentition (odontogenic infection or HSV)
b. Mucous membrane ulcers (inflammatory bowel disease, Behçet disease, or HSV [most commonly located on the vermillion border])
c. Tongue tenderness (amyloidosis or temporal arteritis)
4. Abdominal examination.
a. Hepatomegaly (alcoholic liver disease, lymphoma, hepatoma, relapsing fever, Q fever, typhoid fever)
b. Splenomegaly (leukemia, lymphoma, rheumatoid arthritis, sarcoidosis, alcoholic liver disease, endocarditis, CMV, EBV, brucellosis, RMSF, pssittacosis, or typhoid fever). Fever and hepatosplenomegaly in a neutropenia patient should raise concern for hepatosplenic candidiasis.
5. Lymphatic examination. While lymphoma, adult Still disease, Whipple
disease, HIV, toxoplasmosis, CMV, EBV, or tuberculosis present with generalized lymphadenopathy, catscratch disease is usually associated with a localized adenopathy.
6. Musculoskeletal examination.
a. Joint pain (gout or pseudogout, SLE, rheumatoid arthritis, rat-bite fever, Lyme disease, Whipple disease, or brucellosis). Joint pain or arm pain in children associated with raising the arms above the head may suggest Takayasu disease.
b. Calf-tenderness (DVT, polymyositis, or RMSF)
c. Costovertebral tenderness (perinephric abscess or pyelonephritis.
d. Spine
i. Bruit (tumor or AV fistula)
ii. Tenderness (vertebral osteomyelitis, endocarditis, brucellosis, or typhoid fever)
e. Sternal tenderness (leukemia, myeloproliferative disorder, osteomyelitis,or brucellosis)
f. Thigh tenderness (brucellosis or polymyositis)
g. Cartilage tenderness (polychondritis, Raynaud syndrome, or CMV)
h. Trapezius tenderness (subdiaphragmatic abscess)
7. Ophthalmologic examination.
a. Subconjunctival hemorrhage (endocarditis)
b. Uveitis (SLE, Behçet disease, sacoidosis, adult Still disease, or tuberculosis)
c. Conjunctivitis (histoplasmosis, tuberculosis, catscratch disease, chlamydia infection, or SLE)
d. Conjunctival suffusion (leptospirosis, RMSF, or relapsing fever)
e. Dry eyes (Sjogren syndrome, polyarteritis nodosa, SLE, or rheumatoid arthritis)
8. Vital signs. While most vital signs are nonspecific to the cause of FUO, the pulse should increase 15 to 20 beats/min for each 1 degree increase in core body temperature greater than 39°C. A lower than normal increase (or no increase) is termed relative bradycardia. Causes include:
a. Beta-blockers or drug fevers
b. CNS-related disease (eg, hemorrhagic stroke)
c. Typhoid fever
d. Malaria
e. Leptospirosis
f. Psittacosis
C. L aboratory Studies. There is no diagnostic gold standard workup for the etiology of FUO. While the following represents a minimum diagnostic evaluation, laboratory testing or imaging should be guided by findings from a complete history and physical examination.
1. CBC with differential cell count. Leukocytosis may suggest infection or leukemia. Leukopenia may be associated with leukemia, lymphoma, or tuberculosis. Thrombocytosis (greater than 600,000 mm³) may be associated with cancer, bone marrow disease, tuberculosis, or infections with yeast or molds.
2. Peripheral blood film/thick and thin films. Nucleated RBCs in the absence of hemolysis may suggest bone marrow disease. Films may also be helpful to identify morphologic abnormalities, hemolytic changes, Babesia spp, and malaria.
3. Basic metabolic panel. Routinely ordered but nonspecific. An elevated calcium level may suggest cancer or pseudogout. An elevated uric acid level may suggest gout.
4. Liver functions test. Alkaline phosphatase may be most important as it may be elevated with temporal arteritis, thyroiditis, or tuberculosis. Abnormal liver enzymes may also suggest alcoholic liver disease, biliary tract and hepatic cirrhosis, liver abscess, hemochromatosis, EBV, or CMV.
5. TSH. Abnormalities may suggest thyroiditis.
6. Urinalysis and microscopy. Routinely ordered but nonspecific for etiologies of FUO. Blood may suggest glomerulonephritis, urinary tract cancer,and urinary tract infection (especially with pyuria). Pyelonephritis may be suggested by the presence of white blood cell casts.
7. Blood and urine cultures. Routinely ordered as three sets of blood cultures and a clean-catch midstream culture.
8. PSA. Elevations may be associated with prostate cancer, bacterial prostatitis, Cryptococcus, or extra-pulmonary tuberculosis.
9. ESR. Nonspecific test that is elevated with infections (greater than 70 mm/ hr may suggest osteomyelitis) or inflammation (eg, temporal arteritis).
10. Antinuclear antibodies and rheumatoid factor.
11. HIV antibody.
12. CMV serology or serum PCR.
13. EBV heterophil antibody test or serology.
14. Viral hepatitis serology (especially when considering chronic hepatitis B or C infections).
15. Q fever, RMSF, Lyme disease, brucellosis, leptospirosis, Whipple disease, as well as rat-bite fever and catscratch disease serology might
be useful depending on the exposure risk.
16. A skin purified protein derivative (PPD) or interferon gamma release assay (eg, QuantiFERON-TB Gold) is important for tuberculosis screening.
D. R adiography Studies
1. Plain-film chest imaging. A 2-view chest image is routinely ordered that
may be helpful to identify tuberculosis or malignancy.
2. CT scan. Imaging of the abdomen and pelvis with contrast is important early in the evaluation as two of the most common causes of FUO include intra-abdominal abscesses or lymphoproliferative disorders.
3. Echocardiography. Transthoracic (TTE) or transesophageal (TEE) imaging in association with the review of Duke criteria is important for the evaluation of endocarditis (see endocarditis chapter).
4. Ultrasonography. A noninvasive imaging study that may be helpful to evaluate biliary tract or pelvic etiologies for FUO.
5. Venous Doppler study. A noninvasive imaging study that may be helpful to evaluate for venous thrombosis.
V. T reatment. The treatment for FUO consists of identifying the underlying
cause and formulating a treatment plan for that particular condition.
multiple occasions that is greater than 38.3°C (101°F) for more than 3-weeks’ duration despite 1 week of logical diagnostic evaluation in the hospital.
B. R evised Classic FUO Definitions and Further Classifications. A fever lasting more than 3 weeks with recordings greater than 38.3°C (101°F) despite logical diagnostic evaluation during 3 days in the hospital or 3 outpatient clinic evaluations.
1. Classic FUO. Defined above with the most common etiologies within 3 main categories: infection, malignancy, or collagen-vascular disease.
2. Nosocomial FUO. Usually a fever occurring in a patient that has been hospitalized for at least 24 hours without a defined source prior to admission or 3 days of evaluation. The more common etiologies of a nosocomial fever include urinary tract infections, catheter-related infections, pneumonia,Clostridium difficile colitis, pulmonary embolism, DVT, septic thrombophlebitis,
gastrointestinal bleed, or medication-induced fever.
3. Neutropenia FUO. A recurrent or persistent fever in a patient with neutropenia (absolute neutrophil count less than 500 cells/mm³ or 0.5 3 109/L] despite 3 days of logical diagnostic evaluation. The more common etiologies include nosocomial etiologies (as above) as well as opportunistic bacterial infections (see below), aspergillosis, candidiasis (eg, hepatosplenic
candidiasis), or HSV/VZV.
4. HIV-related FUO. A recurrent or persistent fever for greater than 4 weeks in a patient seropositive for HIV despite 3 days of logical diagnostic evaluation in the hospital. The more common etiologies include: Mycobacterium avium-intracellulare complex (MAC), CMV, Pneumocystis jiroveci p., lymphoma, Kaposi sarcoma, toxoplasmosis, cryptococcus, or medications.

II. Ca uses of FUO .While greater than 200 possible causes for FUO have been reported, the following lists are the more common causes to be considered initially.A cause may not be found in as many as 20% to 30% of cases. The causes are listed by the three main etiologic categories:
A. Infection. This group of causes has been estimated to occur in 28% of FUO cases. The etiologies to initially consider include:
1. Tuberculosis (Mycobacterium tuberculosis; pulmonary and extrapulmonary disease.
2. Abdominal or pelvic abscess (most common cause in the elderly age group).
3. Sinusitis (most commonly with chronic infections or hospitalized patients with nasogastric tubes).
4. Dental abscess (usually oral bacterial flora and may or may not be associated with a recent dental procedure).
5. Endocarditis (most commonly culture negative endocarditis).
6. Osteomyelitis (most commonly chronic osteomyelitis).
7. Hepatitis or chronic biliary tract infections
8. Prostatitis (especially with a recent prostate procedure and is characterized by chronic pelvic pain).
9. HIV infection or sexually transmitted disease
10. CMV (cytomegalovirus; especially in immunocompromised patients).
11. EBV (Epstein-Barr virus; especially following posthematopoietic stem cell transplantation).
12. HSV or VZV (herpes simplex virus and varicella-zoster virus; most commonly associated with reactivation infections in immunocompromised patients).
13. Rocky Mountain spotted fever or Lyme disease (Rickettsia rickettsii or Borrelia burgdorferi; usually associated with outdoor activities and a tick bite).
14. Q fever (Coxiella burnetii; associated with exposure to farm animals [cattle, sheep, or goats] and is characterized by flu-like symptoms with fevers, pneumonia, and hepatitis).
15. Brucellosis (Brucella spp; associated with exposure to animals [goats, sheep, bison, or swine] and is characterized by intermittent fevers, gastrointestinal symptoms [eg, nausea, abdominal pain], and joint effusions).
16. Leptospirosis (Leptospira interrogans; usually associated with rodents or colonized dogs [the organism resides in the renal tubules and is shed in the urine] during recreational activities and is characterized by malaise, headaches, myalgias, abdominal pain, and conjunctival
erythema).
17. Psittacosis (Chlamydophila psittaci; usually associated with birds, especially parrots, and is characterized by fevers, chills, malaise, myalgias, and nonproductive cough).
18. Malaria (Plasmodium spp; transmitted by the Anopheles mosquito and usually characterized by periodic fevers, chills, and rigors).
19. Leishmaniasis (a group of obligate intracellular parasites that are transmitted by sand flies [genera Phlebotomus and Lutzomyia]; commonly associated with cutaneous lesions [eg, a necrotic ulcer] but can be associated with fevers, chills, diarrhea, weight loss, and hepatosplenomegaly).
20. Babesiosis (Babesia spp; an intraerythrocyte parasitic infection transmitted by the bite of an Ixodes tick and characterized by fevers, chills,night sweats, fatigue, weakness, and anemia).
21. Enteric fever (Salmonella enterica, serovar Typhi; associated with travel and characterized by fevers, headaches, myalgias, malaise, and gastrointestinal pain).
22. Toxoplasmosis (Toxoplasma gondii; most commonly a reactivation infection in immunocompromised patients).
23. Rat-bite fever (Streptobacillus moniliformis; patients have an exposure to rats and the disorder is characterized by fevers, headaches, chills, polyarthralgias, and a maculopapular rash on the hands and/or feet).
24. Catscratch disease (Bartonella henselae; a disorder characterized by fevers and localized adenopathy with an exposure to cats).
25. Whipple disease (Tropheryma whippelii; a disorder characterized by
fevers, arthralgia, abdominal pain, chronic diarrhea, weight loss, and generalized lymphadenopathy).
26. Mycobacterium avium-intracellulare complex (MAC; usually associated with fevers and cavitary pulmonary disease in immunocompromised patients).
27. Pneumocystis jirovecii pneumonia (almost exclusively associated with acute hypoxic pneumonia in immunocompromised patients, especially acquired immune deficiency syndrome patients with a CD4 cell count below 200 cells/mm3).
28. Cryptococcus neoformans (commonly associated with chronic corticosteroid use or immunocompromised patients and usually presents as fevers with meningitis or pulmonary pneumonia).
29. Aspergillosis (Aspergillus spp; opportunistic pathogens that can be associated with fevers and pulmonary cavities or endocarditis).
30. Candidiasis (Candida spp; opportunistic pathogens that can be associated with fevers and catheter infections, endocarditis, or hepatosplenic candidiasis).
B. Malignancy. This group typically accounts for 17% of cases. The etiologies to
initially consider include:
1. Leukemia (more commonly chronic leukemia).
2. Lymphoma (most common cause in this group—Hodgkin and non- Hodgkin lymphoma).
3. Renal cell carcinoma.
4. Colorectal cancers.
5. Myelodysplastic syndrome.
6. Pancreatic carcinoma (most commonly not associated with biliary or pancreatic duct obstruction).
7. Metastatic cancer with or without known primary.
C. C ollagen Vascular Disease. This group is estimated to account for 21% of
cases. The etiologies to initially consider include:
1. Temporal arteritis (more common over the age of 50).
2. Rheumatoid arthritis.
3. SLE.
4. Polymyalgia rheumatic.
5. Vasculitis.
6. Polychondritis.
7. Polymyositis.
8. Adult Still disease or adult juvenile rheumatoid arthritis.
9. Sjögren syndrome or Behçet syndrome.
D. Miscellaneous. This group accounts for 5% to 10% of cases. The etiologies
to initially consider include:
1. Crohn disease or ulcerative colitis.
2. Thyroiditis.
3. Sarcoidosis.
4. Amyloidosis.
5. Gout or pseudogout.
6. Addison disease.
7. Hemochromatosis.
8. Medications. The fever usually resolves within 2 to 5 days of discontinuation of the medication. More common medications to consider include:
a. Antibiotics (penicillin, cephalosporin, sulfonamide, tetracycline, and rifampin)
b. Anticonvulsants (phenytoin, carbamazepine, and barbiturates)
c. Antihistamines
d. Nonsteroidal anti-inflammatory drugs (NSAIDs)
e. Iodine and iodide agents (eg, contrast dye)
III. C linical Manif estations of FUO . While documentation of fever is required to establish the diagnosis of FUO, there is no significant relationship between the fever pattern and underlying etiology. However, some associations have been suggested:
A. D ouble Quotidian Fever. Defined as a fever with two peaks within 24 hours;
conditions to consider include endocarditis, malaria, military Mycobacterium
tuberculosis, adult Still disease, and leishmaniasis.
B. S ustained Fever. Defined as a continuously elevated temperature and most
commonly associated with CNS injury (eg, stroke, bleed, etc) or pneumonia
(most commonly secondary to a gram-positive pathogen).
C. Pel-Ebstein Fever. A daily fever that resolves only to reoccur again with a
similar pattern; consider Hodgkin disease.
D. Periodic or Relapsing Fever. Consider endocarditis, malaria, lymphoma, Lyme disease, RMSF, or rat-bite fever.
E. E arly Morning Fever Spike. Consider Mycobacterium tuberculosis, polyarteritis nodosa, brucellosis, or salmonellosis. In general, there are no classic symptoms or signs pathognomonic for a particular FUO etiology, and conditions or causes may be a typical or atypical presentation for a particular disease. It should also be emphasized that no symptom or sign be regarded as irrelevant in a patient suspected of FUO.
IV. App roach to the Patient with FUO
A. H istory. The most important initial approach to the patient with FUO is documenting the fever and recording a complete, accurate, and comprehensive history. Physicians must be meticulous and systematic when obtaining information for the following key elements:
1. Age. Certain illnesses may be more likely associated with particular age groups (eg, malignancy, temporal arteritis, and intra-abdominal abscess may be more likely in persons over the age of 50).
2. History of present illness. While most patients exhibit atypical manifestation, it is important to establish in chronological fashion the onset of symptoms and events that may be related to the fever.
3. Past medical history. This area should focus on any recent or chronic medical illness or infection; and any prior diagnosis of malignancy; and any prior surgery or complication related to surgery; and any implanted prosthetic device, prosthetic valve, pacemaker or implantable defibrillator,
cosmetic implanted surgical device, indwelling venous catheter, or implanted vascular graft.
4. Medications. A complete list of prescription, over-the-counter, and herbal medications should be documented. Drug-related fevers are more common in the elderly and HIV seropositive patient groups.
5. Allergies. Medication allergies may suggest a drug fever while environmental allergies may suggest an atopic condition.
6. Social history. This should include information about the patient’s country of origin, immigration status, prior country or state of residence, travel history (with relevant exposure, vaccination, and prophylaxis history), vaccination status, occupation and occupational risks, smoking status,alcohol and drug exposure, hobbies or leisure activities, pet or animal exposure, dietary (usual or unusual) habits, and sexual activity.
7. Family history. It is important to establish any recent or prior illness in family members and any unusual hereditary cause for fever (eg, familial Mediterranean fever).
B. Physical Examination. A complete physical examination should be performed with attention to all body systems. While physicians should be meticulous and conduct the examination in a systematic approach, repeat examinations are often helpful as diagnostic clues may be either atypical or obscure for the cause of the FUO. Areas of the physical examination that require careful attention and common associations include:
1. Dermatologic examination.
a. Rose spot (typhoid or psittacosis)
b. Hyperpigmentation (hemochromatosis, Addison disease, or Whipple disease)
c. Petechial rash (RMSF)
d. Erythema multiforme (Lyme disease)
e. Vesicular rash on an erythematous base (HSV or VZV)
2. Cardiovascular examination. A new diastolic murmur or change with existing murmur may suggest endocarditis or atrial myxoma.
3. Oral-pharyngeal examination.
a. Gingivitis and/or poor dentition (odontogenic infection or HSV)
b. Mucous membrane ulcers (inflammatory bowel disease, Behçet disease, or HSV [most commonly located on the vermillion border])
c. Tongue tenderness (amyloidosis or temporal arteritis)
4. Abdominal examination.
a. Hepatomegaly (alcoholic liver disease, lymphoma, hepatoma, relapsing fever, Q fever, typhoid fever)
b. Splenomegaly (leukemia, lymphoma, rheumatoid arthritis, sarcoidosis, alcoholic liver disease, endocarditis, CMV, EBV, brucellosis, RMSF, pssittacosis, or typhoid fever). Fever and hepatosplenomegaly in a neutropenia patient should raise concern for hepatosplenic candidiasis.
5. Lymphatic examination. While lymphoma, adult Still disease, Whipple
disease, HIV, toxoplasmosis, CMV, EBV, or tuberculosis present with generalized lymphadenopathy, catscratch disease is usually associated with a localized adenopathy.
6. Musculoskeletal examination.
a. Joint pain (gout or pseudogout, SLE, rheumatoid arthritis, rat-bite fever, Lyme disease, Whipple disease, or brucellosis). Joint pain or arm pain in children associated with raising the arms above the head may suggest Takayasu disease.
b. Calf-tenderness (DVT, polymyositis, or RMSF)
c. Costovertebral tenderness (perinephric abscess or pyelonephritis.
d. Spine
i. Bruit (tumor or AV fistula)
ii. Tenderness (vertebral osteomyelitis, endocarditis, brucellosis, or typhoid fever)
e. Sternal tenderness (leukemia, myeloproliferative disorder, osteomyelitis,or brucellosis)
f. Thigh tenderness (brucellosis or polymyositis)
g. Cartilage tenderness (polychondritis, Raynaud syndrome, or CMV)
h. Trapezius tenderness (subdiaphragmatic abscess)
7. Ophthalmologic examination.
a. Subconjunctival hemorrhage (endocarditis)
b. Uveitis (SLE, Behçet disease, sacoidosis, adult Still disease, or tuberculosis)
c. Conjunctivitis (histoplasmosis, tuberculosis, catscratch disease, chlamydia infection, or SLE)
d. Conjunctival suffusion (leptospirosis, RMSF, or relapsing fever)
e. Dry eyes (Sjogren syndrome, polyarteritis nodosa, SLE, or rheumatoid arthritis)
8. Vital signs. While most vital signs are nonspecific to the cause of FUO, the pulse should increase 15 to 20 beats/min for each 1 degree increase in core body temperature greater than 39°C. A lower than normal increase (or no increase) is termed relative bradycardia. Causes include:
a. Beta-blockers or drug fevers
b. CNS-related disease (eg, hemorrhagic stroke)
c. Typhoid fever
d. Malaria
e. Leptospirosis
f. Psittacosis
C. L aboratory Studies. There is no diagnostic gold standard workup for the etiology of FUO. While the following represents a minimum diagnostic evaluation, laboratory testing or imaging should be guided by findings from a complete history and physical examination.
1. CBC with differential cell count. Leukocytosis may suggest infection or leukemia. Leukopenia may be associated with leukemia, lymphoma, or tuberculosis. Thrombocytosis (greater than 600,000 mm³) may be associated with cancer, bone marrow disease, tuberculosis, or infections with yeast or molds.
2. Peripheral blood film/thick and thin films. Nucleated RBCs in the absence of hemolysis may suggest bone marrow disease. Films may also be helpful to identify morphologic abnormalities, hemolytic changes, Babesia spp, and malaria.
3. Basic metabolic panel. Routinely ordered but nonspecific. An elevated calcium level may suggest cancer or pseudogout. An elevated uric acid level may suggest gout.
4. Liver functions test. Alkaline phosphatase may be most important as it may be elevated with temporal arteritis, thyroiditis, or tuberculosis. Abnormal liver enzymes may also suggest alcoholic liver disease, biliary tract and hepatic cirrhosis, liver abscess, hemochromatosis, EBV, or CMV.
5. TSH. Abnormalities may suggest thyroiditis.
6. Urinalysis and microscopy. Routinely ordered but nonspecific for etiologies of FUO. Blood may suggest glomerulonephritis, urinary tract cancer,and urinary tract infection (especially with pyuria). Pyelonephritis may be suggested by the presence of white blood cell casts.
7. Blood and urine cultures. Routinely ordered as three sets of blood cultures and a clean-catch midstream culture.
8. PSA. Elevations may be associated with prostate cancer, bacterial prostatitis, Cryptococcus, or extra-pulmonary tuberculosis.
9. ESR. Nonspecific test that is elevated with infections (greater than 70 mm/ hr may suggest osteomyelitis) or inflammation (eg, temporal arteritis).
10. Antinuclear antibodies and rheumatoid factor.
11. HIV antibody.
12. CMV serology or serum PCR.
13. EBV heterophil antibody test or serology.
14. Viral hepatitis serology (especially when considering chronic hepatitis B or C infections).
15. Q fever, RMSF, Lyme disease, brucellosis, leptospirosis, Whipple disease, as well as rat-bite fever and catscratch disease serology might
be useful depending on the exposure risk.
16. A skin purified protein derivative (PPD) or interferon gamma release assay (eg, QuantiFERON-TB Gold) is important for tuberculosis screening.
D. R adiography Studies
1. Plain-film chest imaging. A 2-view chest image is routinely ordered that
may be helpful to identify tuberculosis or malignancy.
2. CT scan. Imaging of the abdomen and pelvis with contrast is important early in the evaluation as two of the most common causes of FUO include intra-abdominal abscesses or lymphoproliferative disorders.
3. Echocardiography. Transthoracic (TTE) or transesophageal (TEE) imaging in association with the review of Duke criteria is important for the evaluation of endocarditis (see endocarditis chapter).
4. Ultrasonography. A noninvasive imaging study that may be helpful to evaluate biliary tract or pelvic etiologies for FUO.
5. Venous Doppler study. A noninvasive imaging study that may be helpful to evaluate for venous thrombosis.
V. T reatment. The treatment for FUO consists of identifying the underlying
cause and formulating a treatment plan for that particular condition.
Tag :
Fever.Fever Unknown Origin,
Fever of Unknown Origin.Causes,signs,symptoms,treatment.
I. Introduction.A. C lassic Fever of Unknown Origin (FUO ) Definition. A temperature record on
multiple occasions that is greater than 38.3°C (101°F) for more than 3-weeks’ duration despite 1 week of logical diagnostic evaluation in the hospital.
B. R evised Classic FUO Definitions and Further Classifications. A fever lasting more than 3 weeks with recordings greater than 38.3°C (101°F) despite logical diagnostic evaluation during 3 days in the hospital or 3 outpatient clinic evaluations.
1. Classic FUO. Defined above with the most common etiologies within 3 main categories: infection, malignancy, or collagen-vascular disease.
2. Nosocomial FUO. Usually a fever occurring in a patient that has been hospitalized for at least 24 hours without a defined source prior to admission or 3 days of evaluation. The more common etiologies of a nosocomial fever include urinary tract infections, catheter-related infections, pneumonia,Clostridium difficile colitis, pulmonary embolism, DVT, septic thrombophlebitis,
gastrointestinal bleed, or medication-induced fever.
3. Neutropenia FUO. A recurrent or persistent fever in a patient with neutropenia (absolute neutrophil count less than 500 cells/mm³ or 0.5 3 109/L] despite 3 days of logical diagnostic evaluation. The more common etiologies include nosocomial etiologies (as above) as well as opportunistic bacterial infections (see below), aspergillosis, candidiasis (eg, hepatosplenic
candidiasis), or HSV/VZV.
4. HIV-related FUO. A recurrent or persistent fever for greater than 4 weeks in a patient seropositive for HIV despite 3 days of logical diagnostic evaluation in the hospital. The more common etiologies include: Mycobacterium avium-intracellulare complex (MAC), CMV, Pneumocystis jiroveci p., lymphoma, Kaposi sarcoma, toxoplasmosis, cryptococcus, or medications.
II. Ca uses of FUO .While greater than 200 possible causes for FUO have been reported, the following lists are the more common causes to be considered initially.A cause may not be found in as many as 20% to 30% of cases. The causes are listed by the three main etiologic categories:
A. Infection. This group of causes has been estimated to occur in 28% of FUO cases. The etiologies to initially consider include:
1. Tuberculosis (Mycobacterium tuberculosis; pulmonary and extrapulmonary disease.
2. Abdominal or pelvic abscess (most common cause in the elderly age group).
3. Sinusitis (most commonly with chronic infections or hospitalized patients with nasogastric tubes).
4. Dental abscess (usually oral bacterial flora and may or may not be associated with a recent dental procedure).
5. Endocarditis (most commonly culture negative endocarditis).
6. Osteomyelitis (most commonly chronic osteomyelitis).
7. Hepatitis or chronic biliary tract infections
8. Prostatitis (especially with a recent prostate procedure and is characterized by chronic pelvic pain).
9. HIV infection or sexually transmitted disease
10. CMV (cytomegalovirus; especially in immunocompromised patients).
11. EBV (Epstein-Barr virus; especially following posthematopoietic stem cell transplantation).
12. HSV or VZV (herpes simplex virus and varicella-zoster virus; most commonly associated with reactivation infections in immunocompromised patients).
13. Rocky Mountain spotted fever or Lyme disease (Rickettsia rickettsii or Borrelia burgdorferi; usually associated with outdoor activities and a tick bite).
14. Q fever (Coxiella burnetii; associated with exposure to farm animals [cattle, sheep, or goats] and is characterized by flu-like symptoms with fevers, pneumonia, and hepatitis).
15. Brucellosis (Brucella spp; associated with exposure to animals [goats, sheep, bison, or swine] and is characterized by intermittent fevers, gastrointestinal symptoms [eg, nausea, abdominal pain], and joint effusions).
16. Leptospirosis (Leptospira interrogans; usually associated with rodents or colonized dogs [the organism resides in the renal tubules and is shed in the urine] during recreational activities and is characterized by malaise, headaches, myalgias, abdominal pain, and conjunctival
erythema).
17. Psittacosis (Chlamydophila psittaci; usually associated with birds, especially parrots, and is characterized by fevers, chills, malaise, myalgias, and nonproductive cough).
18. Malaria (Plasmodium spp; transmitted by the Anopheles mosquito and usually characterized by periodic fevers, chills, and rigors).
19. Leishmaniasis (a group of obligate intracellular parasites that are transmitted by sand flies [genera Phlebotomus and Lutzomyia]; commonly associated with cutaneous lesions [eg, a necrotic ulcer] but can be associated with fevers, chills, diarrhea, weight loss, and hepatosplenomegaly).
20. Babesiosis (Babesia spp; an intraerythrocyte parasitic infection transmitted by the bite of an Ixodes tick and characterized by fevers, chills,night sweats, fatigue, weakness, and anemia).
21. Enteric fever (Salmonella enterica, serovar Typhi; associated with travel and characterized by fevers, headaches, myalgias, malaise, and gastrointestinal pain).
22. Toxoplasmosis (Toxoplasma gondii; most commonly a reactivation infection in immunocompromised patients).
23. Rat-bite fever (Streptobacillus moniliformis; patients have an exposure to rats and the disorder is characterized by fevers, headaches, chills, polyarthralgias, and a maculopapular rash on the hands and/or feet).
24. Catscratch disease (Bartonella henselae; a disorder characterized by fevers and localized adenopathy with an exposure to cats).
25. Whipple disease (Tropheryma whippelii; a disorder characterized by
fevers, arthralgia, abdominal pain, chronic diarrhea, weight loss, and generalized lymphadenopathy).
26. Mycobacterium avium-intracellulare complex (MAC; usually associated with fevers and cavitary pulmonary disease in immunocompromised patients).
27. Pneumocystis jirovecii pneumonia (almost exclusively associated with acute hypoxic pneumonia in immunocompromised patients, especially acquired immune deficiency syndrome patients with a CD4 cell count below 200 cells/mm3).
28. Cryptococcus neoformans (commonly associated with chronic corticosteroid use or immunocompromised patients and usually presents as fevers with meningitis or pulmonary pneumonia).
29. Aspergillosis (Aspergillus spp; opportunistic pathogens that can be associated with fevers and pulmonary cavities or endocarditis).
30. Candidiasis (Candida spp; opportunistic pathogens that can be associated with fevers and catheter infections, endocarditis, or hepatosplenic candidiasis).
B. Malignancy. This group typically accounts for 17% of cases. The etiologies to
initially consider include:
1. Leukemia (more commonly chronic leukemia).
2. Lymphoma (most common cause in this group—Hodgkin and non- Hodgkin lymphoma).
3. Renal cell carcinoma.
4. Colorectal cancers.
5. Myelodysplastic syndrome.
6. Pancreatic carcinoma (most commonly not associated with biliary or pancreatic duct obstruction).
7. Metastatic cancer with or without known primary.
C. C ollagen Vascular Disease. This group is estimated to account for 21% of
cases. The etiologies to initially consider include:
1. Temporal arteritis (more common over the age of 50).
2. Rheumatoid arthritis.
3. SLE.
4. Polymyalgia rheumatic.
5. Vasculitis.
6. Polychondritis.
7. Polymyositis.
8. Adult Still disease or adult juvenile rheumatoid arthritis.
9. Sjögren syndrome or Behçet syndrome.
D. Miscellaneous. This group accounts for 5% to 10% of cases. The etiologies
to initially consider include:
1. Crohn disease or ulcerative colitis.
2. Thyroiditis.
3. Sarcoidosis.
4. Amyloidosis.
5. Gout or pseudogout.
6. Addison disease.
7. Hemochromatosis.
8. Medications. The fever usually resolves within 2 to 5 days of discontinuation of the medication. More common medications to consider include:
a. Antibiotics (penicillin, cephalosporin, sulfonamide, tetracycline, and rifampin)
b. Anticonvulsants (phenytoin, carbamazepine, and barbiturates)
c. Antihistamines
d. Nonsteroidal anti-inflammatory drugs (NSAIDs)
e. Iodine and iodide agents (eg, contrast dye)
III. C linical Manif estations of FUO . While documentation of fever is required to establish the diagnosis of FUO, there is no significant relationship between the fever pattern and underlying etiology. However, some associations have been suggested:
A. D ouble Quotidian Fever. Defined as a fever with two peaks within 24 hours;
conditions to consider include endocarditis, malaria, military Mycobacterium
tuberculosis, adult Still disease, and leishmaniasis.
B. S ustained Fever. Defined as a continuously elevated temperature and most
commonly associated with CNS injury (eg, stroke, bleed, etc) or pneumonia
(most commonly secondary to a gram-positive pathogen).
C. Pel-Ebstein Fever. A daily fever that resolves only to reoccur again with a
similar pattern; consider Hodgkin disease.
D. Periodic or Relapsing Fever. Consider endocarditis, malaria, lymphoma, Lyme disease, RMSF, or rat-bite fever.
E. E arly Morning Fever Spike. Consider Mycobacterium tuberculosis, polyarteritis nodosa, brucellosis, or salmonellosis. In general, there are no classic symptoms or signs pathognomonic for a particular FUO etiology, and conditions or causes may be a typical or atypical presentation for a particular disease. It should also be emphasized that no symptom or sign be regarded as irrelevant in a patient suspected of FUO.
IV. App roach to the Patient with FUO
A. H istory. The most important initial approach to the patient with FUO is documenting the fever and recording a complete, accurate, and comprehensive history. Physicians must be meticulous and systematic when obtaining information for the following key elements:
1. Age. Certain illnesses may be more likely associated with particular age groups (eg, malignancy, temporal arteritis, and intra-abdominal abscess may be more likely in persons over the age of 50).
2. History of present illness. While most patients exhibit atypical manifestation, it is important to establish in chronological fashion the onset of symptoms and events that may be related to the fever.
3. Past medical history. This area should focus on any recent or chronic medical illness or infection; and any prior diagnosis of malignancy; and any prior surgery or complication related to surgery; and any implanted prosthetic device, prosthetic valve, pacemaker or implantable defibrillator,
cosmetic implanted surgical device, indwelling venous catheter, or implanted vascular graft.
4. Medications. A complete list of prescription, over-the-counter, and herbal medications should be documented. Drug-related fevers are more common in the elderly and HIV seropositive patient groups.
5. Allergies. Medication allergies may suggest a drug fever while environmental allergies may suggest an atopic condition.
6. Social history. This should include information about the patient’s country of origin, immigration status, prior country or state of residence, travel history (with relevant exposure, vaccination, and prophylaxis history), vaccination status, occupation and occupational risks, smoking status,alcohol and drug exposure, hobbies or leisure activities, pet or animal exposure, dietary (usual or unusual) habits, and sexual activity.
7. Family history. It is important to establish any recent or prior illness in family members and any unusual hereditary cause for fever (eg, familial Mediterranean fever).
B. Physical Examination. A complete physical examination should be performed with attention to all body systems. While physicians should be meticulous and conduct the examination in a systematic approach, repeat examinations are often helpful as diagnostic clues may be either atypical or obscure for the cause of the FUO. Areas of the physical examination that require careful attention and common associations include:
1. Dermatologic examination.
a. Rose spot (typhoid or psittacosis)
b. Hyperpigmentation (hemochromatosis, Addison disease, or Whipple disease)
c. Petechial rash (RMSF)
d. Erythema multiforme (Lyme disease)
e. Vesicular rash on an erythematous base (HSV or VZV)
2. Cardiovascular examination. A new diastolic murmur or change with existing murmur may suggest endocarditis or atrial myxoma.
3. Oral-pharyngeal examination.
a. Gingivitis and/or poor dentition (odontogenic infection or HSV)
b. Mucous membrane ulcers (inflammatory bowel disease, Behçet disease, or HSV [most commonly located on the vermillion border])
c. Tongue tenderness (amyloidosis or temporal arteritis)
4. Abdominal examination.
a. Hepatomegaly (alcoholic liver disease, lymphoma, hepatoma, relapsing fever, Q fever, typhoid fever)
b. Splenomegaly (leukemia, lymphoma, rheumatoid arthritis, sarcoidosis, alcoholic liver disease, endocarditis, CMV, EBV, brucellosis, RMSF, pssittacosis, or typhoid fever). Fever and hepatosplenomegaly in a neutropenia patient should raise concern for hepatosplenic candidiasis.
5. Lymphatic examination. While lymphoma, adult Still disease, Whipple
disease, HIV, toxoplasmosis, CMV, EBV, or tuberculosis present with generalized lymphadenopathy, catscratch disease is usually associated with a localized adenopathy.
6. Musculoskeletal examination.
a. Joint pain (gout or pseudogout, SLE, rheumatoid arthritis, rat-bite fever, Lyme disease, Whipple disease, or brucellosis). Joint pain or arm pain in children associated with raising the arms above the head may suggest Takayasu disease.
b. Calf-tenderness (DVT, polymyositis, or RMSF)
c. Costovertebral tenderness (perinephric abscess or pyelonephritis.
d. Spine
i. Bruit (tumor or AV fistula)
ii. Tenderness (vertebral osteomyelitis, endocarditis, brucellosis, or typhoid fever)
e. Sternal tenderness (leukemia, myeloproliferative disorder, osteomyelitis,or brucellosis)
f. Thigh tenderness (brucellosis or polymyositis)
g. Cartilage tenderness (polychondritis, Raynaud syndrome, or CMV)
h. Trapezius tenderness (subdiaphragmatic abscess)
7. Ophthalmologic examination.
a. Subconjunctival hemorrhage (endocarditis)
b. Uveitis (SLE, Behçet disease, sacoidosis, adult Still disease, or tuberculosis)
c. Conjunctivitis (histoplasmosis, tuberculosis, catscratch disease, chlamydia infection, or SLE)
d. Conjunctival suffusion (leptospirosis, RMSF, or relapsing fever)
e. Dry eyes (Sjogren syndrome, polyarteritis nodosa, SLE, or rheumatoid arthritis)
8. Vital signs. While most vital signs are nonspecific to the cause of FUO, the pulse should increase 15 to 20 beats/min for each 1 degree increase in core body temperature greater than 39°C. A lower than normal increase (or no increase) is termed relative bradycardia. Causes include:
a. Beta-blockers or drug fevers
b. CNS-related disease (eg, hemorrhagic stroke)
c. Typhoid fever
d. Malaria
e. Leptospirosis
f. Psittacosis
C. L aboratory Studies. There is no diagnostic gold standard workup for the etiology of FUO. While the following represents a minimum diagnostic evaluation, laboratory testing or imaging should be guided by findings from a complete history and physical examination.
1. CBC with differential cell count. Leukocytosis may suggest infection or leukemia. Leukopenia may be associated with leukemia, lymphoma, or tuberculosis. Thrombocytosis (greater than 600,000 mm³) may be associated with cancer, bone marrow disease, tuberculosis, or infections with yeast or molds.
2. Peripheral blood film/thick and thin films. Nucleated RBCs in the absence of hemolysis may suggest bone marrow disease. Films may also be helpful to identify morphologic abnormalities, hemolytic changes, Babesia spp, and malaria.
3. Basic metabolic panel. Routinely ordered but nonspecific. An elevated calcium level may suggest cancer or pseudogout. An elevated uric acid level may suggest gout.
4. Liver functions test. Alkaline phosphatase may be most important as it may be elevated with temporal arteritis, thyroiditis, or tuberculosis. Abnormal liver enzymes may also suggest alcoholic liver disease, biliary tract and hepatic cirrhosis, liver abscess, hemochromatosis, EBV, or CMV.
5. TSH. Abnormalities may suggest thyroiditis.
6. Urinalysis and microscopy. Routinely ordered but nonspecific for etiologies of FUO. Blood may suggest glomerulonephritis, urinary tract cancer,and urinary tract infection (especially with pyuria). Pyelonephritis may be suggested by the presence of white blood cell casts.
7. Blood and urine cultures. Routinely ordered as three sets of blood cultures and a clean-catch midstream culture.
8. PSA. Elevations may be associated with prostate cancer, bacterial prostatitis, Cryptococcus, or extra-pulmonary tuberculosis.
9. ESR. Nonspecific test that is elevated with infections (greater than 70 mm/ hr may suggest osteomyelitis) or inflammation (eg, temporal arteritis).
10. Antinuclear antibodies and rheumatoid factor.
11. HIV antibody.
12. CMV serology or serum PCR.
13. EBV heterophil antibody test or serology.
14. Viral hepatitis serology (especially when considering chronic hepatitis B or C infections).
15. Q fever, RMSF, Lyme disease, brucellosis, leptospirosis, Whipple disease, as well as rat-bite fever and catscratch disease serology might
be useful depending on the exposure risk.
16. A skin purified protein derivative (PPD) or interferon gamma release assay (eg, QuantiFERON-TB Gold) is important for tuberculosis screening.
D. R adiography Studies
1. Plain-film chest imaging. A 2-view chest image is routinely ordered that
may be helpful to identify tuberculosis or malignancy.
2. CT scan. Imaging of the abdomen and pelvis with contrast is important early in the evaluation as two of the most common causes of FUO include intra-abdominal abscesses or lymphoproliferative disorders.
3. Echocardiography. Transthoracic (TTE) or transesophageal (TEE) imaging in association with the review of Duke criteria is important for the evaluation of endocarditis (see endocarditis chapter).
4. Ultrasonography. A noninvasive imaging study that may be helpful to evaluate biliary tract or pelvic etiologies for FUO.
5. Venous Doppler study. A noninvasive imaging study that may be helpful to evaluate for venous thrombosis.
V. T reatment. The treatment for FUO consists of identifying the underlying
cause and formulating a treatment plan for that particular condition.
multiple occasions that is greater than 38.3°C (101°F) for more than 3-weeks’ duration despite 1 week of logical diagnostic evaluation in the hospital.
B. R evised Classic FUO Definitions and Further Classifications. A fever lasting more than 3 weeks with recordings greater than 38.3°C (101°F) despite logical diagnostic evaluation during 3 days in the hospital or 3 outpatient clinic evaluations.
1. Classic FUO. Defined above with the most common etiologies within 3 main categories: infection, malignancy, or collagen-vascular disease.
2. Nosocomial FUO. Usually a fever occurring in a patient that has been hospitalized for at least 24 hours without a defined source prior to admission or 3 days of evaluation. The more common etiologies of a nosocomial fever include urinary tract infections, catheter-related infections, pneumonia,Clostridium difficile colitis, pulmonary embolism, DVT, septic thrombophlebitis,
gastrointestinal bleed, or medication-induced fever.
3. Neutropenia FUO. A recurrent or persistent fever in a patient with neutropenia (absolute neutrophil count less than 500 cells/mm³ or 0.5 3 109/L] despite 3 days of logical diagnostic evaluation. The more common etiologies include nosocomial etiologies (as above) as well as opportunistic bacterial infections (see below), aspergillosis, candidiasis (eg, hepatosplenic
candidiasis), or HSV/VZV.
4. HIV-related FUO. A recurrent or persistent fever for greater than 4 weeks in a patient seropositive for HIV despite 3 days of logical diagnostic evaluation in the hospital. The more common etiologies include: Mycobacterium avium-intracellulare complex (MAC), CMV, Pneumocystis jiroveci p., lymphoma, Kaposi sarcoma, toxoplasmosis, cryptococcus, or medications.
II. Ca uses of FUO .While greater than 200 possible causes for FUO have been reported, the following lists are the more common causes to be considered initially.A cause may not be found in as many as 20% to 30% of cases. The causes are listed by the three main etiologic categories:
A. Infection. This group of causes has been estimated to occur in 28% of FUO cases. The etiologies to initially consider include:
1. Tuberculosis (Mycobacterium tuberculosis; pulmonary and extrapulmonary disease.
2. Abdominal or pelvic abscess (most common cause in the elderly age group).
3. Sinusitis (most commonly with chronic infections or hospitalized patients with nasogastric tubes).
4. Dental abscess (usually oral bacterial flora and may or may not be associated with a recent dental procedure).
5. Endocarditis (most commonly culture negative endocarditis).
6. Osteomyelitis (most commonly chronic osteomyelitis).
7. Hepatitis or chronic biliary tract infections
8. Prostatitis (especially with a recent prostate procedure and is characterized by chronic pelvic pain).
9. HIV infection or sexually transmitted disease
10. CMV (cytomegalovirus; especially in immunocompromised patients).
11. EBV (Epstein-Barr virus; especially following posthematopoietic stem cell transplantation).
12. HSV or VZV (herpes simplex virus and varicella-zoster virus; most commonly associated with reactivation infections in immunocompromised patients).
13. Rocky Mountain spotted fever or Lyme disease (Rickettsia rickettsii or Borrelia burgdorferi; usually associated with outdoor activities and a tick bite).
14. Q fever (Coxiella burnetii; associated with exposure to farm animals [cattle, sheep, or goats] and is characterized by flu-like symptoms with fevers, pneumonia, and hepatitis).
15. Brucellosis (Brucella spp; associated with exposure to animals [goats, sheep, bison, or swine] and is characterized by intermittent fevers, gastrointestinal symptoms [eg, nausea, abdominal pain], and joint effusions).
16. Leptospirosis (Leptospira interrogans; usually associated with rodents or colonized dogs [the organism resides in the renal tubules and is shed in the urine] during recreational activities and is characterized by malaise, headaches, myalgias, abdominal pain, and conjunctival
erythema).
17. Psittacosis (Chlamydophila psittaci; usually associated with birds, especially parrots, and is characterized by fevers, chills, malaise, myalgias, and nonproductive cough).
18. Malaria (Plasmodium spp; transmitted by the Anopheles mosquito and usually characterized by periodic fevers, chills, and rigors).
19. Leishmaniasis (a group of obligate intracellular parasites that are transmitted by sand flies [genera Phlebotomus and Lutzomyia]; commonly associated with cutaneous lesions [eg, a necrotic ulcer] but can be associated with fevers, chills, diarrhea, weight loss, and hepatosplenomegaly).
20. Babesiosis (Babesia spp; an intraerythrocyte parasitic infection transmitted by the bite of an Ixodes tick and characterized by fevers, chills,night sweats, fatigue, weakness, and anemia).
21. Enteric fever (Salmonella enterica, serovar Typhi; associated with travel and characterized by fevers, headaches, myalgias, malaise, and gastrointestinal pain).
22. Toxoplasmosis (Toxoplasma gondii; most commonly a reactivation infection in immunocompromised patients).
23. Rat-bite fever (Streptobacillus moniliformis; patients have an exposure to rats and the disorder is characterized by fevers, headaches, chills, polyarthralgias, and a maculopapular rash on the hands and/or feet).
24. Catscratch disease (Bartonella henselae; a disorder characterized by fevers and localized adenopathy with an exposure to cats).
25. Whipple disease (Tropheryma whippelii; a disorder characterized by
fevers, arthralgia, abdominal pain, chronic diarrhea, weight loss, and generalized lymphadenopathy).
26. Mycobacterium avium-intracellulare complex (MAC; usually associated with fevers and cavitary pulmonary disease in immunocompromised patients).
27. Pneumocystis jirovecii pneumonia (almost exclusively associated with acute hypoxic pneumonia in immunocompromised patients, especially acquired immune deficiency syndrome patients with a CD4 cell count below 200 cells/mm3).
28. Cryptococcus neoformans (commonly associated with chronic corticosteroid use or immunocompromised patients and usually presents as fevers with meningitis or pulmonary pneumonia).
29. Aspergillosis (Aspergillus spp; opportunistic pathogens that can be associated with fevers and pulmonary cavities or endocarditis).
30. Candidiasis (Candida spp; opportunistic pathogens that can be associated with fevers and catheter infections, endocarditis, or hepatosplenic candidiasis).
B. Malignancy. This group typically accounts for 17% of cases. The etiologies to
initially consider include:
1. Leukemia (more commonly chronic leukemia).
2. Lymphoma (most common cause in this group—Hodgkin and non- Hodgkin lymphoma).
3. Renal cell carcinoma.
4. Colorectal cancers.
5. Myelodysplastic syndrome.
6. Pancreatic carcinoma (most commonly not associated with biliary or pancreatic duct obstruction).
7. Metastatic cancer with or without known primary.
C. C ollagen Vascular Disease. This group is estimated to account for 21% of
cases. The etiologies to initially consider include:
1. Temporal arteritis (more common over the age of 50).
2. Rheumatoid arthritis.
3. SLE.
4. Polymyalgia rheumatic.
5. Vasculitis.
6. Polychondritis.
7. Polymyositis.
8. Adult Still disease or adult juvenile rheumatoid arthritis.
9. Sjögren syndrome or Behçet syndrome.
D. Miscellaneous. This group accounts for 5% to 10% of cases. The etiologies
to initially consider include:
1. Crohn disease or ulcerative colitis.
2. Thyroiditis.
3. Sarcoidosis.
4. Amyloidosis.
5. Gout or pseudogout.
6. Addison disease.
7. Hemochromatosis.
8. Medications. The fever usually resolves within 2 to 5 days of discontinuation of the medication. More common medications to consider include:
a. Antibiotics (penicillin, cephalosporin, sulfonamide, tetracycline, and rifampin)
b. Anticonvulsants (phenytoin, carbamazepine, and barbiturates)
c. Antihistamines
d. Nonsteroidal anti-inflammatory drugs (NSAIDs)
e. Iodine and iodide agents (eg, contrast dye)
III. C linical Manif estations of FUO . While documentation of fever is required to establish the diagnosis of FUO, there is no significant relationship between the fever pattern and underlying etiology. However, some associations have been suggested:
A. D ouble Quotidian Fever. Defined as a fever with two peaks within 24 hours;
conditions to consider include endocarditis, malaria, military Mycobacterium
tuberculosis, adult Still disease, and leishmaniasis.
B. S ustained Fever. Defined as a continuously elevated temperature and most
commonly associated with CNS injury (eg, stroke, bleed, etc) or pneumonia
(most commonly secondary to a gram-positive pathogen).
C. Pel-Ebstein Fever. A daily fever that resolves only to reoccur again with a
similar pattern; consider Hodgkin disease.
D. Periodic or Relapsing Fever. Consider endocarditis, malaria, lymphoma, Lyme disease, RMSF, or rat-bite fever.
E. E arly Morning Fever Spike. Consider Mycobacterium tuberculosis, polyarteritis nodosa, brucellosis, or salmonellosis. In general, there are no classic symptoms or signs pathognomonic for a particular FUO etiology, and conditions or causes may be a typical or atypical presentation for a particular disease. It should also be emphasized that no symptom or sign be regarded as irrelevant in a patient suspected of FUO.
IV. App roach to the Patient with FUO
A. H istory. The most important initial approach to the patient with FUO is documenting the fever and recording a complete, accurate, and comprehensive history. Physicians must be meticulous and systematic when obtaining information for the following key elements:
1. Age. Certain illnesses may be more likely associated with particular age groups (eg, malignancy, temporal arteritis, and intra-abdominal abscess may be more likely in persons over the age of 50).
2. History of present illness. While most patients exhibit atypical manifestation, it is important to establish in chronological fashion the onset of symptoms and events that may be related to the fever.
3. Past medical history. This area should focus on any recent or chronic medical illness or infection; and any prior diagnosis of malignancy; and any prior surgery or complication related to surgery; and any implanted prosthetic device, prosthetic valve, pacemaker or implantable defibrillator,
cosmetic implanted surgical device, indwelling venous catheter, or implanted vascular graft.
4. Medications. A complete list of prescription, over-the-counter, and herbal medications should be documented. Drug-related fevers are more common in the elderly and HIV seropositive patient groups.
5. Allergies. Medication allergies may suggest a drug fever while environmental allergies may suggest an atopic condition.
6. Social history. This should include information about the patient’s country of origin, immigration status, prior country or state of residence, travel history (with relevant exposure, vaccination, and prophylaxis history), vaccination status, occupation and occupational risks, smoking status,alcohol and drug exposure, hobbies or leisure activities, pet or animal exposure, dietary (usual or unusual) habits, and sexual activity.
7. Family history. It is important to establish any recent or prior illness in family members and any unusual hereditary cause for fever (eg, familial Mediterranean fever).
B. Physical Examination. A complete physical examination should be performed with attention to all body systems. While physicians should be meticulous and conduct the examination in a systematic approach, repeat examinations are often helpful as diagnostic clues may be either atypical or obscure for the cause of the FUO. Areas of the physical examination that require careful attention and common associations include:
1. Dermatologic examination.
a. Rose spot (typhoid or psittacosis)
b. Hyperpigmentation (hemochromatosis, Addison disease, or Whipple disease)
c. Petechial rash (RMSF)
d. Erythema multiforme (Lyme disease)
e. Vesicular rash on an erythematous base (HSV or VZV)
2. Cardiovascular examination. A new diastolic murmur or change with existing murmur may suggest endocarditis or atrial myxoma.
3. Oral-pharyngeal examination.
a. Gingivitis and/or poor dentition (odontogenic infection or HSV)
b. Mucous membrane ulcers (inflammatory bowel disease, Behçet disease, or HSV [most commonly located on the vermillion border])
c. Tongue tenderness (amyloidosis or temporal arteritis)
4. Abdominal examination.
a. Hepatomegaly (alcoholic liver disease, lymphoma, hepatoma, relapsing fever, Q fever, typhoid fever)
b. Splenomegaly (leukemia, lymphoma, rheumatoid arthritis, sarcoidosis, alcoholic liver disease, endocarditis, CMV, EBV, brucellosis, RMSF, pssittacosis, or typhoid fever). Fever and hepatosplenomegaly in a neutropenia patient should raise concern for hepatosplenic candidiasis.
5. Lymphatic examination. While lymphoma, adult Still disease, Whipple
disease, HIV, toxoplasmosis, CMV, EBV, or tuberculosis present with generalized lymphadenopathy, catscratch disease is usually associated with a localized adenopathy.
6. Musculoskeletal examination.
a. Joint pain (gout or pseudogout, SLE, rheumatoid arthritis, rat-bite fever, Lyme disease, Whipple disease, or brucellosis). Joint pain or arm pain in children associated with raising the arms above the head may suggest Takayasu disease.
b. Calf-tenderness (DVT, polymyositis, or RMSF)
c. Costovertebral tenderness (perinephric abscess or pyelonephritis.
d. Spine
i. Bruit (tumor or AV fistula)
ii. Tenderness (vertebral osteomyelitis, endocarditis, brucellosis, or typhoid fever)
e. Sternal tenderness (leukemia, myeloproliferative disorder, osteomyelitis,or brucellosis)
f. Thigh tenderness (brucellosis or polymyositis)
g. Cartilage tenderness (polychondritis, Raynaud syndrome, or CMV)
h. Trapezius tenderness (subdiaphragmatic abscess)
7. Ophthalmologic examination.
a. Subconjunctival hemorrhage (endocarditis)
b. Uveitis (SLE, Behçet disease, sacoidosis, adult Still disease, or tuberculosis)
c. Conjunctivitis (histoplasmosis, tuberculosis, catscratch disease, chlamydia infection, or SLE)
d. Conjunctival suffusion (leptospirosis, RMSF, or relapsing fever)
e. Dry eyes (Sjogren syndrome, polyarteritis nodosa, SLE, or rheumatoid arthritis)
8. Vital signs. While most vital signs are nonspecific to the cause of FUO, the pulse should increase 15 to 20 beats/min for each 1 degree increase in core body temperature greater than 39°C. A lower than normal increase (or no increase) is termed relative bradycardia. Causes include:
a. Beta-blockers or drug fevers
b. CNS-related disease (eg, hemorrhagic stroke)
c. Typhoid fever
d. Malaria
e. Leptospirosis
f. Psittacosis
C. L aboratory Studies. There is no diagnostic gold standard workup for the etiology of FUO. While the following represents a minimum diagnostic evaluation, laboratory testing or imaging should be guided by findings from a complete history and physical examination.
1. CBC with differential cell count. Leukocytosis may suggest infection or leukemia. Leukopenia may be associated with leukemia, lymphoma, or tuberculosis. Thrombocytosis (greater than 600,000 mm³) may be associated with cancer, bone marrow disease, tuberculosis, or infections with yeast or molds.
2. Peripheral blood film/thick and thin films. Nucleated RBCs in the absence of hemolysis may suggest bone marrow disease. Films may also be helpful to identify morphologic abnormalities, hemolytic changes, Babesia spp, and malaria.
3. Basic metabolic panel. Routinely ordered but nonspecific. An elevated calcium level may suggest cancer or pseudogout. An elevated uric acid level may suggest gout.
4. Liver functions test. Alkaline phosphatase may be most important as it may be elevated with temporal arteritis, thyroiditis, or tuberculosis. Abnormal liver enzymes may also suggest alcoholic liver disease, biliary tract and hepatic cirrhosis, liver abscess, hemochromatosis, EBV, or CMV.
5. TSH. Abnormalities may suggest thyroiditis.
6. Urinalysis and microscopy. Routinely ordered but nonspecific for etiologies of FUO. Blood may suggest glomerulonephritis, urinary tract cancer,and urinary tract infection (especially with pyuria). Pyelonephritis may be suggested by the presence of white blood cell casts.
7. Blood and urine cultures. Routinely ordered as three sets of blood cultures and a clean-catch midstream culture.
8. PSA. Elevations may be associated with prostate cancer, bacterial prostatitis, Cryptococcus, or extra-pulmonary tuberculosis.
9. ESR. Nonspecific test that is elevated with infections (greater than 70 mm/ hr may suggest osteomyelitis) or inflammation (eg, temporal arteritis).
10. Antinuclear antibodies and rheumatoid factor.
11. HIV antibody.
12. CMV serology or serum PCR.
13. EBV heterophil antibody test or serology.
14. Viral hepatitis serology (especially when considering chronic hepatitis B or C infections).
15. Q fever, RMSF, Lyme disease, brucellosis, leptospirosis, Whipple disease, as well as rat-bite fever and catscratch disease serology might
be useful depending on the exposure risk.
16. A skin purified protein derivative (PPD) or interferon gamma release assay (eg, QuantiFERON-TB Gold) is important for tuberculosis screening.
D. R adiography Studies
1. Plain-film chest imaging. A 2-view chest image is routinely ordered that
may be helpful to identify tuberculosis or malignancy.
2. CT scan. Imaging of the abdomen and pelvis with contrast is important early in the evaluation as two of the most common causes of FUO include intra-abdominal abscesses or lymphoproliferative disorders.
3. Echocardiography. Transthoracic (TTE) or transesophageal (TEE) imaging in association with the review of Duke criteria is important for the evaluation of endocarditis (see endocarditis chapter).
4. Ultrasonography. A noninvasive imaging study that may be helpful to evaluate biliary tract or pelvic etiologies for FUO.
5. Venous Doppler study. A noninvasive imaging study that may be helpful to evaluate for venous thrombosis.
V. T reatment. The treatment for FUO consists of identifying the underlying
cause and formulating a treatment plan for that particular condition.
Tag :
Fever.Fever Unknown Origin,
Primary Hypertension.
Overview.The majority of patients with hypertension have primary (or essential) hypertension. The pathogenesis of primary hypertension is not completely understood; at best, it is known that there are risk factors and conditions that may contribute
to development of primary hypertension. This lack of understanding precludes a true cure of primary hypertension. Rather, the clinician is limited to reducing the patient’s BP to goal values through lifestyle modification and prescribing antihypertensive medications. With this approach, BP can often be reduced to normotensive levels. In the majority of cases, the only treatment is long-term BP control. In some patients, hypertension may be secondary to other, coexisting conditions, and in these cases the cause of the hypertension is better understood. Usually, the elevated BP can be resolved or improved with correction to the underlying condition, and this becomes the focus of treatment. Approximately 5% of patients with hypertension have a secondary form of hypertension.
Determinants of blood pressure .The BP is determined by a combination of factors, including CO, total body fluid volume, and resistance of blood moving through the arterial system. In addition, many environmental factors alter the function of organ systems, thereby generating a complex interaction of multiple factors, all adding to the difficulty in determining the cause(s) of primary hypertension.
Cardiac output and blood volume.CO is the amount of blood pumped by the heart over a period of time and is determined by the speed at which the heart beats (heart rate) and the amount of blood pumped by each heart beat (stroke volume). Left ventricular stroke volume is the difference between the volume of blood that has filled the left ventricle at the end of diastole (end diastolic volume, EDV) and the amount of blood left in the left ventricle immediately following systolic contraction (end systolic volume, ESV). Stroke volume is dependent on the preload, the afterload, and the contractility of the heart:
A) Preload is the amount of stretch of the cardiac muscle due to blood filling the heart, which is controlloed by the EDV filled by venous return from circulation. Any factor that alters the returning volume will alter the EDV and the preload. Changes in the EDV affect the stroke volume and, ultimately, CO. A more rapid heart rate, for example, diminishes the amount of blood filling the ventricles and thus decreases preload. B)Afterload is back pressure from the arteries near the heart because of blood movement. Afterload is relatively constant and does not normally make a large contribution to changes in stroke volume. In patients with hypertension, however, afterload is more important, as elevated BP reduces the amount of blood ejected from the heart with each heart contraction. This leaves more blood in the heart after each contraction, raising the ESV and thus reducing
the stroke volume. C) An extrinsic factor affecting stroke volume is cardiac contractility. Cardiac contractility is termed extrinsic because it does not depend on myocardial stretch. Increased contractility increases the force and amount of blood ejected with each heart beat. This reduces the ESV, increasing the stroke volume. Contractility is increased due to cytosolic increase in calcium ions prior tocontraction.
The components that regulate CO rely on a number of sensors sensitive to hemodynamic changes including baroreceptors and chemoreceptors located within arteries and receptors in skeletal muscle that sense contractions.Baroreceptors are mechanoreceptors that sense changes in vessel wall stretch and produce a rapid response to alterations in BP. They act as a buffering system to moderate normal short-term changes in BP. In hypertension, the increased stretching of arterial walls activates these receptors, causing inhibition of the vasomotor center and resultant reduction in heart rate (to lower CO) and vasodilation (to decrease SVR). These changes reduce the BP. If the BP is too low,
these receptors sense the reduction in arterial pressure and increase the CO and stimulate vasoconstriction. The long-term function of baroreceptors is not known. Baroreceptors can be reset and may no longer respond to changes in stretching associated with increased BP, which may occur in hypertension.Blood volume is another important factor in BP level. Regulation of blood volume is a long-term modulator of CO. Blood volume influences venous pressure and ventricular filling, which causes changes in EDV and stroke volume. BP is directly tied to blood volume; when blood volume increases, BP rises.The kidneys have an important role in controlling blood and fluid volume. They can directly alter blood volume by increasing the filtration of fluid and reducing sodium retention and the fluid that accompanies it. Indirectly, the kidneys can regulate the renin–angiotensin–aldosterone system (RAAS) to change BP and ultimately increase the blood volume.
A partial list of mechanisms that can influence cardiac output or systemic vascular resistance. This list only includes a few neurotransmitters and hormonal signaling molecules.
A) Norepinephrine/epinephrine B ) Angiotensin II C ) Endothelin D) Nitric oxide E) Atrial natriuretic peptide/brain natriuretic peptide F) Acetylcholine G) Prostaglandins H) Aldosterone I) Bradykinin J) Vasopressin
Systemic vascular resistance.SVR is the resistance to blood flow in the arterial tree. Arteries are composed of endothelial cells, vascular smooth muscle cells, and connective tissue. The intrinsic myogenic tone of the vascular smooth muscle and the sympathetic nervous system (SNS) control the diameter of the vessel, which influences the SVR. The nervous system and the endothelial cells play a major role in modifying smooth muscle cell tone. (See Table 3.1 for a partial list of factors that can alter SVR and CO.) There are several vasodilators that reduce SVR, notably nitric oxide. Nitric oxide activates guanylate cyclase in smooth muscle cells, resulting in an increase in cyclic guanosine monophosphate (GMP) and vessel relaxation. Constriction of smooth muscle cells, however, increases SVR. This system prevents BP from falling too low and increases BP in response to stress or activity. Principal vasoconstrictors are angiotensin (AT) II (produced in response to release of renin by the kidney) and endothelin-1 (ET-1) produced by endothelial cells. ET-1 binds to receptors of vascular smooth muscle cells to activate voltage-dependent calcium channels. AT II binds the G-protein coupled receptor AT1 to increase cytoplasmic calcium concentrations.
Blood pressure regulation. Many physiological systems alter CO and SVR and thus regulate BP. Systemic and local hormones, metabolites, and neurotransmitters all contribute to signaling pathways that affect CO and SVR. The SNS and the RAAS play a particularly important role in BP management.
Sympathetic nervous system The SNS can alter SVR and CO and thus regulate BP in response to stimuli (Figures). The parasympathetic nervous system mostly functions to downregulate the system and the main parasympathetic neurotransmitter,
acetylcholine, is responsible for reducing heart rate. The SNS counteracts the relaxed state that dominates under parasympathetic activity to prepare the body for activity or stress. It is the SNS, through its main neurotransmitter, epinephrine, that results in many of the changes leading to increases in BP and, as such, it is an
important target in treating hypertension. The SNS signals via adrenergic receptors, which respond to the neurotransmitter
norepinephrine (NE) (and epinephrine). Both alpha- and beta-adrenergic receptors, and several subclasses of each receptor, are involved. Alpha1, alpha2, and beta1 adrenergic receptors are the most important receptors in increasing and regulating
BP. Stimulation of postsynaptic alpha1 and alpha2 adrenergic receptors located
Sympathetic nervous system and blood pressure regulation pathways.

on smooth muscle cells causes vasoconstriction of the vessels. Activation of beta1 adrenergic receptors in heart muscle causes increased heart rate and increases the amount of calcium in the muscle cells, thereby increasing cardiac contractility. CO is raised due to increased stroke volume and heart rate. Beta1 adrenergic receptors within the kidney, when stimulated, signal for release of renin, resulting in the production of the vasoconstrictor AT II. This stimulation of the SNS increases CO and SVR, leading to increased BP.(Fig. )Pathological consequences of activation of the renin–angiotensin–aldosterone system.


Fig) Interaction between the renin–angiotensin–aldosterone
system and the sympathetic nervous system at the kidney.


Renin–angiotensin–aldosterone system Blood and fluid volume influence CO and are dependent on sodium regulation by the kidneys (Figure 3.3). The kidneys play a key role in controlling BP by causing changes in fluid volume, sodium homeostasis, and SVR. There are many different systems that regulate these factors, including the RAAS. This is a hormonal system that works to regulate BP and fluid volume through several mechanisms.
In response to decreased blood fluid volume, the kidneys release the proteolytic enzyme renin into circulation. Renin cleaves angiotensinogen in the blood stream into AT I. AT I is further processed into AT II by angiotensin-converting enzyme (ACE). AT II is an active molecule and can stimulate two subtypes of receptors. Stimulation of the AT1 receptor subclass can cause several changes that counteract low fluid levels and, in turn, increase BP. The first mechanism to increase blood fluid volume is through sodium retention. The AT II–AT1 receptor pathway acts
directly on the proximal renal tube and causes sodium reabsorption. AT1 receptor activation also stimulates aldosterone release, causing further salt retention by the kidney. Both of these mechanisms lead to fluid retention and increased BP. AT1 receptor stimulation causes changes in blood vessels via vasoconstriction. AT II, signaling through AT1 receptors, is known to stimulate the SNS. This leads to changes in CO and SVR. All of these functions of AT II stimulation of the AT1 subclass of receptors lead to an increase in systemic BP.
Primary hypertension:risk factors and blood pressure regulation
Although the cause of primary hypertension is unknown, there are many risk factors associated with hypertension. Children with hypertensive parents are more than twice as likely to develop hypertension, suggesting that there is a genetic component. This is supported by epidemiological evidence suggesting that up to 30% of BP variation in the overall population is due to genetic abnormalities. Hypertension is also more prevalent in the USA in the non-Hispanic black population compared with the non-Hispanic white or Mexican American population.Hypertension as a whole is more severe in the black population compared with other races. There are also many factors associated with lifestyle and environment that may contribute to an increased risk of developing hypertension (below2.1). Diet can enhance the susceptibility to develop, and once developed, sustain hypertension.
For example, excess sodium intake and alcohol have both been linked to an increased likelihood of hypertension. Obesity is also a major risk factor, and in the elderly it is the main risk factor associated with the onset of hypertension.Psychological stress and lack of physical activity are also linked with elevated BP. While it is likely that all of these risk factors contribute to hypertension, the
contribution of each risk factor depends on individual patient susceptibility.
Sodium intake and primary hypertension.Sodium balance correlates with raised BP. Primary hypertension is more common
in populations that consume higher amounts of sodium, especially if the average sodium intake is 100 mEq/day or more, but it is rare in populations that consume less than an average of 50 mEq/day. Reducing sodium intake can have a beneficial effect on BP. Sodium reduction from 170–100 mEq/day can reduce systolic BP
2.1 Some of the factors that may influence the development of primary hypertension.
OO Increased sodium intake
OO Increased body mass
OO Increased alcohol intake
OO Increased psychological stress
OO Decreased physical activity
OO Genetic predisposition
OO Reduced potassium intake
OO Reduced calcium intake
by 5 mmHg and diastolic BP by 3 mmHg on average. JNC 7 recommends that all persons with a sodium intake of 100–150 mEq/day should reduce their sodium intake to less than 100 mEq/day. Changes in BP due to excess sodium intake reflect sodium sensitivity. Sodium sensitivity varies among individuals, and it increases with age or obesity. Non- Hispanic blacks are also more susceptible to sodium sensitivity and individuals with
renal dysfunction have greater sodium sensitivity than people with normal kidney function. The relationship between sodium and BP is not ully understood, but may be related to fluid volume. Excess sodium intake requires the kidneys to filter more sodium out of the blood stream. If the level of sodium overwhelms the ability
of the kidneys to filter sodium, sodium retention occurs,contributing directly to excess fluid volume and, ultimately, hypertension. It is also possible that excess sodium causes other changes in the body, such as activating signaling pathways,which can lead to inappropriate vasodilation or vasoconstriction. Sodium also
exacerbates other risk factors such as microalbuminuria and dyslipidemia.
Genetics and primary hypertension. Many genes have been linked to hypertension (Table 3.3). One example of a single gene mutation leading to hypertension is Liddle’s syndrome, caused by the dominant gain of function mutation in the sodium channel. This mutation prevents the degradation of the channel and leads to overactivity. The early and severe hypertension common in Liddle’s syndrome is due to excessive sodium reabsorption, which causes systemic volume overload.Primary hypertension, however, is unlikely to be due to a single gene mutation.There have been many genes associated with an increased risk of hypertension,but the individual contributions of each gene are currently unknown. Based on animal models, there is evidence that genes active in the kidney are the largest contributors to genetic-based hypertension. There is evidence that the AT, adducin,and connexin 40 genes have a pathogenetic role in high BP.Stress and primary hypertension.
Stress is believed to contribute to the development of hypertension. Physiological stress leads to activation of the SNS and can lead to vasoconstriction and changes to SVR. Stress associated with being seen in medical clinics (white-coat hypertension)is one of the leading causes of pseudoresistant hypertension. Over time, stress can lead to long-term hypertension; patients with repeated physiological stress have a higher incidence of elevated BP.
One way to combat stress is to increase physical activity. Lack of physical activity can contribute to essential hypertension by leading to higher stress levels, greater risk of obesity, and reduced cardiovascular function. Several epidemiological studies have demonstrated a link between low physical activity and higher BP,
mainly through the contribution of increased body mass in less active persons.
Hypertension.
INTRODUCTION TO HYPERTENSION:
hypertension
overview
It has been recognized that the heart and blood vessels play a critical role in maintaining bodily functions through the provision of circulation to vital organs. The cardiovascular system sustains the metabolic demands of all organs, with the pumping action of the heart being responsible for generating and maintaining an adequate blood supply to all the tissues. This pumping activity of the heart determines cardiac output (CO) which, coupled with systemic vascular resistance (SVR), determines the blood pressure (BP) and blood flow. CO or SVR, or both, can be affected by a number of factors, resulting in an alteration in the normal regulation of BP. Hypertension refers to an increase in intra-arterial pressure. Currently, most guidelines around the world define hypertension as systolic BP levels in excess of 140 mmHg or diastolic BP levels greater than 90 mmHg; normal BP is 120/80 mmHg or lower. Any BP level between those two ranges is now called either prehypertension or borderline hypertension. Large numbers of people both in developed and developing societies throughout the world will eventually develop hypertension at some point in their lifetime
Prevalence of
hypertension as a percentage
of the population from the
National Health and Nutrition
Examination Survey observations.
(Adapted from Wright JD, Hughes
JP, Ostchega Y et al. (2011)
Mean systolic and diastolic
blood pressure in adults aged 18
and over in the United States,
2001–2008. Natl Health Stat Report


There are many factors that influence the balance between CO and SVR. CO is dependent on both the function (pumping action) of the heart and the circulating volume of blood. In turn, blood volume is strongly influenced by sodium regulation and the fluid handling abilities of the kidneys. Thus, the kidneys play a major role in maintaining fluid and sodium homeostasis, with impairment of kidney function (even of modest degree) causing significant aberrations their ability to regulate fluid volume. SVR is dependent on several characteristics of the blood vessels, including wall thickness and vasomotor tone. In addition, metabolic factors, local environment, and humeral milieu can all affect and influence SVR. In about 5–10% of cases, hypertension is secondary to a specific cause. In such
cases of secondary hypertension, correction of the underlying abnormality will often ameliorate or even completely correct hypertension. In the remaining 90% of patients with essential or primary hypertension, there may be no obvious cause. Many factors are known to contribute to hypertension including certain lifestyle changes, age, environmental factors, and genetic predisposition. In most cases, even with the varied or unknown etiology of disease, hypertension can be treated or greatly improved with combinations of medication and non-pharmacological treatments. Effective treatment of hypertension is important because successful therapy reduces the risk of morbidity and mortality associated with hypertension. The initial stages of hypertension are usually asymptomatic, therefore without routine BP monitoring hypertension can go undetected for many years. This
makes hypertension truly a ‘silent killer’. Some of the complications associated with hypertension, many of which affect the cardiovascular system at a very early stage, are listed in Table. For example, hypertension can cause cardiac myocardial hypertrophy and vascular remodeling. If left untreated, patients with hypertension are at an increased risk of death from cardiovascular disease (CVD), including stroke, myocardial infarction, heart failure, and other complications. Treatment of hypertension can stop progression of disease and may even reverse target organ damage (TOD). This prospect highlights the need for aggressive treatment of hypertension to reduce and maintain BP at
normal levels.
Some health complications associated with hypertension.

Hypertension and cardiovascular disease:
CVD is rapidly emerging as a major global health hazard. In the USA it is now the leading cause of death, with almost one million deaths attributed to CVD annually. CVD includes coronary heart disease, stroke, heart failure, and other related conditions and mainly affects persons over 60 years of age. Hypertension is the major risk factor associated with the development of premature CVD, ahead of cigarette smoking, diabetes, and dyslipidemia. The effect of BP on cardiovascular risk is progressive and continuous as the pressure increases, such that patients with high BP levels are at greater risk of developing congestive heart failure (CHF) than those with low BP levels . The risk is conferred on all age groups and with any combination of additional risk factors, which can exacerbate morbidity and mortality. However, even with all of the evidence that hypertension is a contributing factor to CVD, mortality directly caused by hypertension can be difficult to determine. The use of death certificates to determine total numbers of deaths associated with a particular condition is based on a record of the immediate cause of death (e.g. heart failure or stroke), which underestimates the underlying influence of hyperten Cardiovascular event rates in people with normal blood pressure (N), white-coat hypertension
(WCH), and sustained hypertension (SH). (Adapted from Pierdomenico SD, Lapenna D, Di
Mascio R et al. (2008) Short- and long-term risk of cardiovascular events in white-coat hypertension.

Cardiovascular risk within the range of ‘normal’ blood pressure (from the Framingham Heart Study). (Adapted from Ramachandran SV, Larson MG, Leip EP et al. (2007) Impact of high-normal blood pressure on the risk of cardiovascular disease.


Risk of cardiovascular disease associated with hypertension.
According to the Framingham Heart Study, hypertension in men is the primary cause of coronary heart disease that results in disability and death. In a global study of patients (both male and female) in over 50 countries, it was estimated that nearly 20% of the risk of the first myocardial infarction (MI) could be attributed entirely to hypertension. In women, mortality as a consequence of hypertension is more likely to be due to stroke. Indeed, hypertension is the most important risk factor
for predicting ischemic stroke and intracerebral hemorrhage
Hypertension onset: progression and complicatio
 Systolic blood pressure and morbitity (from the Framingham Heart Study). (Adapted from Dawber TR, Kannel WB, Revotskie N et al. (1962) The epidemiology of coronary heart disease – the Framingham enquiry.
Systolic blood pressure and morbitity (from the Framingham Heart Study). (Adapted from Dawber TR, Kannel WB, Revotskie N et al. (1962) The epidemiology of coronary heart disease – the Framingham enquiry.


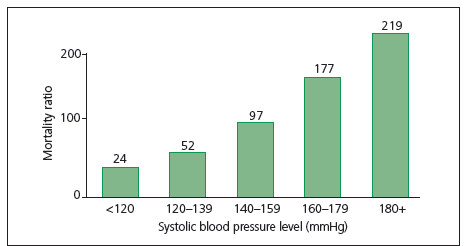
Cardiovascular disease and prehypertension.
Increased risk of CVD is not limited to patients who have hypertension by traditional
definitions. The risk of developing CVD is related to the BP level ( in Figure).
Studies of the population at large and patients with documented CVD suggest
that this relationship begins at BP levels above 115/75 mmHg, which is considered
Risk of stroke mortality (from the Multiple
Risk Factors Intervention Trial [MRFIT] cohort).
(Adapted from Neaton JD, Kuller L, Stamler J et al.
(1995) Impact of systolic and diastolic blood
pressure on cardiovascular mortality. In: Hypertension:
Pathophysiology, Diagnosis, and Management.


Fig. Risk of developing chronic heart disease
(from the Framingham Heart Study). (Adapted from
Dawber TR, Kannel WB, Revotskie N et al. (1962)
The epidemiology of coronary heart disease – the
Framingham enquiry.

Fig. Risk of chronic heart disease (from the
Multiple Risk Factors Intervention Trial [MRFIT]
cohort). (Adapted from Neaton JD, Kuller L,
Stamler J et al. (1995) Impact of systolic and
diastolic blood pressure on cardiovascular mortality.
In: Hypertension: Pathophysiology, Diagnosis, and
Management.
 ‘normal’ BP. This range of BP levels between normal patients (120/80 mmHg)
‘normal’ BP. This range of BP levels between normal patients (120/80 mmHg)

and hypertensive patients (140/90 mmHg) is referred to as prehypertension, and
patients with BP levels within this range have an increased risk of developing
coronary heart disease or having a MI compared with patients with a normal BP.
A study limited to women also suggests that having a stroke is more likely in the
prehypertension population than in the population with normal BP. However,
direct conclusions from these data are complex because prehypertensive patients
also tend to have additional CVD risk factors compared with patients with normal
BP. These risk factors include increased body weight, elevated serum cholesterol
level and diabetes mellitus, which add to the difficuty in determining cause and
effect relationships. The best evidence for a relationship between increased BP at
prehypertension levels and CVD is supported by outcomes from antihypertensive
therapy. Treatment with antihypertensive drugs decreases the risk of developing
CVD by about two-thirds compared with untreated patients, even when other risk
factors remain unchanged.
Changes associated with hypertension that can lead to cardiovascular disease.
Diseases of the CV system that are associated with hypertension can be attributed, at least in part, to changes in organ systems as the body attempts to adapt tohigher arterial pressures. Elevated BP leads to structural changes in the arteriolesand the remainder of the vascular tree, referred to as remodeling or hypertrophy, which contribute to damage to other organ systems. Larger vessels undergo
arteriosclerosis in response to the higher sheer stress imposed by hypertension. This correlates with patient age, with older patients having a higher relative risk of arteriosclerosis than younger patients. Hypertension also plays an independent role in atherosclerosis, causing substantial premature morbidity and mortality. When these changes occur in cerebral blood vessels, the risk of stroke is increased. A common abnormality seen in hypertensive patients is left ventricular hypertrophy (LVH), which occurs as a result of thickening in the left ventricular, changes in left ventricular geometry, and an increase in left ventricular mass. LVH is a precursor of heart failure, MI, and cardiac arrhythmias. The majority of patients with CHF have a history of chronic hypertension, with the risk for CHF increased by three times in hypertensive patients compared with people with
normal BP levels.
Prevalence and epidemiology of hypertension
Hypertension in the population.
Hypertension and its associated complications affect a large number of people around the world. A recent National Health and Nutrition Examination Survey (NHANES) estimated that 29–32% of the adult population (age >18 years) in the USA could currently be classified as having hypertension (systolic BP >140 mmHg or diastolic BP >90 mmHg). This prevalence equates to over 60 million people. Perhaps even significant is the finding that an additional 28% of the population has prehypertension. Thus, the majority of the population of the USA has one of the major risk factors for CVD. Global statistics are similar. Currently, 26% of the world population is estimated to have this hypertension, which translates to almost one billion people with this disease. In a recent review studying the worldwide prevalence of hypertension , the lowest prevalence was found in rural India (3.4% in men and 6.8% in women) and the highest prevalence was in Poland (68.9% in men and 72.5% in women). Awareness of hypertension was reported in 46% of the populations
studied, and varied from 25.2% in Korea to 75% in Barbados. Treatment frequently also varied greatly, ranging from 10.7% in Mexico to 66% in Barbados, and BP control (BP <140/90 mmHg while on antihypertensive medication) varied from 5.4% in Korea to 58% in Barbados. Despite recent efforts to control hypertension, these statistics show little improvement in the USA. There has been no significant decrease in the percentage of the population with hypertension in recent decades.
Prevalence of
hypertension in people aged
20 years and older by world
region and sex in 2000 (upper)
and projected for 2025 (lower).
(Adapted from Kearney PM,
Whelton M, Reynolds K et
al. (2005) Global burden
of hypertension: analysis
of worldwide data.


These data have been examined and sorted into different subgroups to try to
identify subpopulations that may be at increased risk (Table 1.2). As BP tends to
rise with aging, it is not surprising that the majority of adults over 60 year of age
have hypertension (67%), compared with just 7% of 18–39 year olds and 31% of
40–59 year olds. The prevalence in men and women was found to be statistically
similar, with nearly 30% of both genders having hypertension. Ethnic breakdown
showed more diversity, with non-Hispanic blacks having the highest prevalence
of hypertension in the population (almost twice the prevalence in Mexican
Americans).
In people with prehypertension (Table 1.3), men are significantly more likely
to have prehypertension than women (34% and 22%, respectively). Ethnic
subgroups are not as dispersed, ranging from 27 to 31% with prehypertension.
Mexican Americans are significantly more likely to have prehypertension than
non-Hispanics. Analysis by age shows that 40–59-year-old people have the highest
prevalence of prehypertension (34%), followed by people aged 18–39 years old
(29%). Only 18% of individuals aged 60 years or older have prehypertension.
This is not surprising as the majority of the population aged 60 years and older
already have BPs in the hypertensive range. These data in the older population are
supported by the observations from the Framingham Heart Study (FHS), which determined the likelihood of a person developing hypertension based on starting
BP and age. The study demonstrated that people aged 65 years or older are 1.5 to
3 times more likely to progress to hypertensive levels compared with those younger
than 65 years. Furthermore, the FHS estimated that 55–65-year-old people had
a greater than 90% chance of developing hypertension during their lifetime
Prevalence of hypertension in subgroups of the adult population in the USA.
(From National Health and Nutrition Examination Survey, 2005–2006.)


Prevalence of prehypertension in subgroups of the adult population in the USA.
(From National Health and Nutrition Examination Survey, 2005–2006.)

Increased risks of cardiovascular disease associated with hypertension
The risk of coronary heart disease, stroke, or cardiovascular mortality increases
with a concurrent increase in BP, starting at 115/75 mmHg. This correlation
appears to be true for patients being treated for hypertension and for those not
being treated. Among patients who already have coronary heart disease, the risk
also increases with rises in BP. A global study with a 25-year follow-up of 12,000
men aged 40–59 years in seven countries estimated that the relative risk of death
increased 1.28-fold for every 10 mmHg increase in systolic BP. The risk of death in
hypertensive patients (at BPs of 140/85 mmHg) was three-fold higher in the USA
and Northern Europe than in Japan and Southern Europe, most likely because
of other contributing factors. These contributing factors, however, can often be
modified in individual patients. It has been estimated that 68% of hypertensive
patients take one or more antihypertensive medications and of these, 64% have
BPs below 140/90 mmHg. There has not been any change in the total percentage
of the population with hypertension in the USA, but many individual patients
have had a reduced risk of CVD by adhering to physician-directed treatment.
Some health complications associated with hypertension
Cardiovascular event rates in people with
normal blood pressure (N), white-coat hypertension
(WCH), and sustained hypertension (SH).
(Adapted from Pierdomenico SD, Lapenna D, Di
Mascio R et al. (2008) Short- and long-term risk of
cardiovascular events in white-coat hypertension.
The public health cost of hypertension:
a global challenge
Several studies have estimated the costs of hypertension and the economic burden
imposed by escalating BP levels in the community. This includes expenditure for
hypertension treatment and care, plus the cost in life and loss of productivity.
Additional studies have tried to determine the cost of treating prehypertensive
patients or ineffective/incorrect treatment of patients. The chronic nature of
hypertension, the large number of people with hypertension, and complications
such as CVD and hypertension-related kidney failure make hypertension highly expensive to both individuals and society.
Financial burden of hypertension in the USA. An estimated 60 million Americans have hypertension, with almost 60 million morehaving prehypertension or non-optimal BP. The current cost estimates for treating
hypertension range from 15 to 30 billion US dollars (USD) per year. The costs
of treating medical conditions associated with hypertension are an additional
87 billion USD. This total includes 30 billion USD for CVD and 57 billion USD
for all other conditions attributable to hypertension. Together, more than 100
billion USD are used to treat hypertension and related conditions, just less than
10% of the total healthcare costs in the USA. Prescription medications, inpatient
treatment, and outpatient treatment account for 90% of the costs directly
related to hypertension, with prescription medication alone accounting for onehalf
of the expenditure. Health preactitioners following established treatment
protocols is important in helping control the costs of hypertension, as deviations
from established protocols are estimated to cost an additional 13 billion USD
annually. Almost 10% of this cost is caused by patients being given inappropriate
prescriptions that are inconsistent with evidenced-based recommendations.
Global financial burden of hypertension
The total cost of hypertension has also been studied globally. These studies have
taken into account costs associated with both hypertension and prehypertension.
The International Society of Hypertension tried to quantify the cost of treating
elevated BP and diseases related to elevated BP (including new cases of ischemic
heart disease and stroke) and estimated that 370 billion USD was spent around the
world in 2001 because of non-optimal BP levels. This global estimate suggests that
the direct cost of non-optimal BP control accounts for about 10% of all healthcare
expenditure. To put this into perspective, because the World Bank defines the
world’s poorest citizens as those living below 1 USD/day, a 370 billion USD
expenditure could raise all of these one billion citizens out of extreme poverty,
highlighting both the magnitude of the expense and the benefits that could be
realized if hypertension could be eliminated.
Other costs of hypertension
There are also ‘indirect costs’ of hypertension, including loss of life and loss of
productivity due to absenteeism, illness, and death. Globally, it has been estimated
that hypertension accounts for 14% of deaths, and approximately 6% of disabilityadjusted
life years (a measure of work time lost to disability) can be attributed
to non-optimal BP. Although such indirect costs are obviously substantial, their
precise financial burden is difficult to estimate.
Total costs of hypertension
The total cost of hypertension, using direct costs (treatment of hypertension
and related medical conditions) and indirect costs (loss of productivity and
life), is estimated at a staggering four trillion USD globally. It is obvious that
hypertension – both controlled and uncontrolled – is a costly and likely unstainable
burden demanding much more attention than it currently receives.







