Halthcare


Showing posts with label introduction to hypertension. Show all posts
Hypertension.
INTRODUCTION TO HYPERTENSION:
hypertension
overview
It has been recognized that the heart and blood vessels play a critical role in maintaining bodily functions through the provision of circulation to vital organs. The cardiovascular system sustains the metabolic demands of all organs, with the pumping action of the heart being responsible for generating and maintaining an adequate blood supply to all the tissues. This pumping activity of the heart determines cardiac output (CO) which, coupled with systemic vascular resistance (SVR), determines the blood pressure (BP) and blood flow. CO or SVR, or both, can be affected by a number of factors, resulting in an alteration in the normal regulation of BP. Hypertension refers to an increase in intra-arterial pressure. Currently, most guidelines around the world define hypertension as systolic BP levels in excess of 140 mmHg or diastolic BP levels greater than 90 mmHg; normal BP is 120/80 mmHg or lower. Any BP level between those two ranges is now called either prehypertension or borderline hypertension. Large numbers of people both in developed and developing societies throughout the world will eventually develop hypertension at some point in their lifetime
Prevalence of
hypertension as a percentage
of the population from the
National Health and Nutrition
Examination Survey observations.
(Adapted from Wright JD, Hughes
JP, Ostchega Y et al. (2011)
Mean systolic and diastolic
blood pressure in adults aged 18
and over in the United States,
2001–2008. Natl Health Stat Report


There are many factors that influence the balance between CO and SVR. CO is dependent on both the function (pumping action) of the heart and the circulating volume of blood. In turn, blood volume is strongly influenced by sodium regulation and the fluid handling abilities of the kidneys. Thus, the kidneys play a major role in maintaining fluid and sodium homeostasis, with impairment of kidney function (even of modest degree) causing significant aberrations their ability to regulate fluid volume. SVR is dependent on several characteristics of the blood vessels, including wall thickness and vasomotor tone. In addition, metabolic factors, local environment, and humeral milieu can all affect and influence SVR. In about 5–10% of cases, hypertension is secondary to a specific cause. In such
cases of secondary hypertension, correction of the underlying abnormality will often ameliorate or even completely correct hypertension. In the remaining 90% of patients with essential or primary hypertension, there may be no obvious cause. Many factors are known to contribute to hypertension including certain lifestyle changes, age, environmental factors, and genetic predisposition. In most cases, even with the varied or unknown etiology of disease, hypertension can be treated or greatly improved with combinations of medication and non-pharmacological treatments. Effective treatment of hypertension is important because successful therapy reduces the risk of morbidity and mortality associated with hypertension. The initial stages of hypertension are usually asymptomatic, therefore without routine BP monitoring hypertension can go undetected for many years. This
makes hypertension truly a ‘silent killer’. Some of the complications associated with hypertension, many of which affect the cardiovascular system at a very early stage, are listed in Table. For example, hypertension can cause cardiac myocardial hypertrophy and vascular remodeling. If left untreated, patients with hypertension are at an increased risk of death from cardiovascular disease (CVD), including stroke, myocardial infarction, heart failure, and other complications. Treatment of hypertension can stop progression of disease and may even reverse target organ damage (TOD). This prospect highlights the need for aggressive treatment of hypertension to reduce and maintain BP at
normal levels.
Some health complications associated with hypertension.

Hypertension and cardiovascular disease:
CVD is rapidly emerging as a major global health hazard. In the USA it is now the leading cause of death, with almost one million deaths attributed to CVD annually. CVD includes coronary heart disease, stroke, heart failure, and other related conditions and mainly affects persons over 60 years of age. Hypertension is the major risk factor associated with the development of premature CVD, ahead of cigarette smoking, diabetes, and dyslipidemia. The effect of BP on cardiovascular risk is progressive and continuous as the pressure increases, such that patients with high BP levels are at greater risk of developing congestive heart failure (CHF) than those with low BP levels . The risk is conferred on all age groups and with any combination of additional risk factors, which can exacerbate morbidity and mortality. However, even with all of the evidence that hypertension is a contributing factor to CVD, mortality directly caused by hypertension can be difficult to determine. The use of death certificates to determine total numbers of deaths associated with a particular condition is based on a record of the immediate cause of death (e.g. heart failure or stroke), which underestimates the underlying influence of hyperten Cardiovascular event rates in people with normal blood pressure (N), white-coat hypertension
(WCH), and sustained hypertension (SH). (Adapted from Pierdomenico SD, Lapenna D, Di
Mascio R et al. (2008) Short- and long-term risk of cardiovascular events in white-coat hypertension.

Cardiovascular risk within the range of ‘normal’ blood pressure (from the Framingham Heart Study). (Adapted from Ramachandran SV, Larson MG, Leip EP et al. (2007) Impact of high-normal blood pressure on the risk of cardiovascular disease.


Risk of cardiovascular disease associated with hypertension.
According to the Framingham Heart Study, hypertension in men is the primary cause of coronary heart disease that results in disability and death. In a global study of patients (both male and female) in over 50 countries, it was estimated that nearly 20% of the risk of the first myocardial infarction (MI) could be attributed entirely to hypertension. In women, mortality as a consequence of hypertension is more likely to be due to stroke. Indeed, hypertension is the most important risk factor
for predicting ischemic stroke and intracerebral hemorrhage
Hypertension onset: progression and complicatio
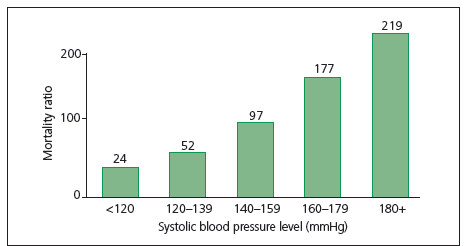
 Systolic blood pressure and morbitity (from the Framingham Heart Study). (Adapted from Dawber TR, Kannel WB, Revotskie N et al. (1962) The epidemiology of coronary heart disease – the Framingham enquiry.
Systolic blood pressure and morbitity (from the Framingham Heart Study). (Adapted from Dawber TR, Kannel WB, Revotskie N et al. (1962) The epidemiology of coronary heart disease – the Framingham enquiry.


Cardiovascular disease and prehypertension.
Increased risk of CVD is not limited to patients who have hypertension by traditional
definitions. The risk of developing CVD is related to the BP level ( in Figure).
Studies of the population at large and patients with documented CVD suggest
that this relationship begins at BP levels above 115/75 mmHg, which is considered
Risk of stroke mortality (from the Multiple
Risk Factors Intervention Trial [MRFIT] cohort).
(Adapted from Neaton JD, Kuller L, Stamler J et al.
(1995) Impact of systolic and diastolic blood
pressure on cardiovascular mortality. In: Hypertension:
Pathophysiology, Diagnosis, and Management.


Fig. Risk of developing chronic heart disease
(from the Framingham Heart Study). (Adapted from
Dawber TR, Kannel WB, Revotskie N et al. (1962)
The epidemiology of coronary heart disease – the
Framingham enquiry.

Fig. Risk of chronic heart disease (from the
Multiple Risk Factors Intervention Trial [MRFIT]
cohort). (Adapted from Neaton JD, Kuller L,
Stamler J et al. (1995) Impact of systolic and
diastolic blood pressure on cardiovascular mortality.
In: Hypertension: Pathophysiology, Diagnosis, and
Management.
 ‘normal’ BP. This range of BP levels between normal patients (120/80 mmHg)
‘normal’ BP. This range of BP levels between normal patients (120/80 mmHg)

and hypertensive patients (140/90 mmHg) is referred to as prehypertension, and
patients with BP levels within this range have an increased risk of developing
coronary heart disease or having a MI compared with patients with a normal BP.
A study limited to women also suggests that having a stroke is more likely in the
prehypertension population than in the population with normal BP. However,
direct conclusions from these data are complex because prehypertensive patients
also tend to have additional CVD risk factors compared with patients with normal
BP. These risk factors include increased body weight, elevated serum cholesterol
level and diabetes mellitus, which add to the difficuty in determining cause and
effect relationships. The best evidence for a relationship between increased BP at
prehypertension levels and CVD is supported by outcomes from antihypertensive
therapy. Treatment with antihypertensive drugs decreases the risk of developing
CVD by about two-thirds compared with untreated patients, even when other risk
factors remain unchanged.
Changes associated with hypertension that can lead to cardiovascular disease.
Diseases of the CV system that are associated with hypertension can be attributed, at least in part, to changes in organ systems as the body attempts to adapt tohigher arterial pressures. Elevated BP leads to structural changes in the arteriolesand the remainder of the vascular tree, referred to as remodeling or hypertrophy, which contribute to damage to other organ systems. Larger vessels undergo
arteriosclerosis in response to the higher sheer stress imposed by hypertension. This correlates with patient age, with older patients having a higher relative risk of arteriosclerosis than younger patients. Hypertension also plays an independent role in atherosclerosis, causing substantial premature morbidity and mortality. When these changes occur in cerebral blood vessels, the risk of stroke is increased. A common abnormality seen in hypertensive patients is left ventricular hypertrophy (LVH), which occurs as a result of thickening in the left ventricular, changes in left ventricular geometry, and an increase in left ventricular mass. LVH is a precursor of heart failure, MI, and cardiac arrhythmias. The majority of patients with CHF have a history of chronic hypertension, with the risk for CHF increased by three times in hypertensive patients compared with people with
normal BP levels.
Prevalence and epidemiology of hypertension
Hypertension in the population.
Hypertension and its associated complications affect a large number of people around the world. A recent National Health and Nutrition Examination Survey (NHANES) estimated that 29–32% of the adult population (age >18 years) in the USA could currently be classified as having hypertension (systolic BP >140 mmHg or diastolic BP >90 mmHg). This prevalence equates to over 60 million people. Perhaps even significant is the finding that an additional 28% of the population has prehypertension. Thus, the majority of the population of the USA has one of the major risk factors for CVD. Global statistics are similar. Currently, 26% of the world population is estimated to have this hypertension, which translates to almost one billion people with this disease. In a recent review studying the worldwide prevalence of hypertension , the lowest prevalence was found in rural India (3.4% in men and 6.8% in women) and the highest prevalence was in Poland (68.9% in men and 72.5% in women). Awareness of hypertension was reported in 46% of the populations
studied, and varied from 25.2% in Korea to 75% in Barbados. Treatment frequently also varied greatly, ranging from 10.7% in Mexico to 66% in Barbados, and BP control (BP <140/90 mmHg while on antihypertensive medication) varied from 5.4% in Korea to 58% in Barbados. Despite recent efforts to control hypertension, these statistics show little improvement in the USA. There has been no significant decrease in the percentage of the population with hypertension in recent decades.
Prevalence of
hypertension in people aged
20 years and older by world
region and sex in 2000 (upper)
and projected for 2025 (lower).
(Adapted from Kearney PM,
Whelton M, Reynolds K et
al. (2005) Global burden
of hypertension: analysis
of worldwide data.


These data have been examined and sorted into different subgroups to try to
identify subpopulations that may be at increased risk (Table 1.2). As BP tends to
rise with aging, it is not surprising that the majority of adults over 60 year of age
have hypertension (67%), compared with just 7% of 18–39 year olds and 31% of
40–59 year olds. The prevalence in men and women was found to be statistically
similar, with nearly 30% of both genders having hypertension. Ethnic breakdown
showed more diversity, with non-Hispanic blacks having the highest prevalence
of hypertension in the population (almost twice the prevalence in Mexican
Americans).
In people with prehypertension (Table 1.3), men are significantly more likely
to have prehypertension than women (34% and 22%, respectively). Ethnic
subgroups are not as dispersed, ranging from 27 to 31% with prehypertension.
Mexican Americans are significantly more likely to have prehypertension than
non-Hispanics. Analysis by age shows that 40–59-year-old people have the highest
prevalence of prehypertension (34%), followed by people aged 18–39 years old
(29%). Only 18% of individuals aged 60 years or older have prehypertension.
This is not surprising as the majority of the population aged 60 years and older
already have BPs in the hypertensive range. These data in the older population are
supported by the observations from the Framingham Heart Study (FHS), which determined the likelihood of a person developing hypertension based on starting
BP and age. The study demonstrated that people aged 65 years or older are 1.5 to
3 times more likely to progress to hypertensive levels compared with those younger
than 65 years. Furthermore, the FHS estimated that 55–65-year-old people had
a greater than 90% chance of developing hypertension during their lifetime
Prevalence of hypertension in subgroups of the adult population in the USA.
(From National Health and Nutrition Examination Survey, 2005–2006.)


Prevalence of prehypertension in subgroups of the adult population in the USA.
(From National Health and Nutrition Examination Survey, 2005–2006.)

Increased risks of cardiovascular disease associated with hypertension
The risk of coronary heart disease, stroke, or cardiovascular mortality increases
with a concurrent increase in BP, starting at 115/75 mmHg. This correlation
appears to be true for patients being treated for hypertension and for those not
being treated. Among patients who already have coronary heart disease, the risk
also increases with rises in BP. A global study with a 25-year follow-up of 12,000
men aged 40–59 years in seven countries estimated that the relative risk of death
increased 1.28-fold for every 10 mmHg increase in systolic BP. The risk of death in
hypertensive patients (at BPs of 140/85 mmHg) was three-fold higher in the USA
and Northern Europe than in Japan and Southern Europe, most likely because
of other contributing factors. These contributing factors, however, can often be
modified in individual patients. It has been estimated that 68% of hypertensive
patients take one or more antihypertensive medications and of these, 64% have
BPs below 140/90 mmHg. There has not been any change in the total percentage
of the population with hypertension in the USA, but many individual patients
have had a reduced risk of CVD by adhering to physician-directed treatment.
Some health complications associated with hypertension
Cardiovascular event rates in people with
normal blood pressure (N), white-coat hypertension
(WCH), and sustained hypertension (SH).
(Adapted from Pierdomenico SD, Lapenna D, Di
Mascio R et al. (2008) Short- and long-term risk of
cardiovascular events in white-coat hypertension.
The public health cost of hypertension:
a global challenge
Several studies have estimated the costs of hypertension and the economic burden
imposed by escalating BP levels in the community. This includes expenditure for
hypertension treatment and care, plus the cost in life and loss of productivity.
Additional studies have tried to determine the cost of treating prehypertensive
patients or ineffective/incorrect treatment of patients. The chronic nature of
hypertension, the large number of people with hypertension, and complications
such as CVD and hypertension-related kidney failure make hypertension highly expensive to both individuals and society.
Financial burden of hypertension in the USA. An estimated 60 million Americans have hypertension, with almost 60 million morehaving prehypertension or non-optimal BP. The current cost estimates for treating
hypertension range from 15 to 30 billion US dollars (USD) per year. The costs
of treating medical conditions associated with hypertension are an additional
87 billion USD. This total includes 30 billion USD for CVD and 57 billion USD
for all other conditions attributable to hypertension. Together, more than 100
billion USD are used to treat hypertension and related conditions, just less than
10% of the total healthcare costs in the USA. Prescription medications, inpatient
treatment, and outpatient treatment account for 90% of the costs directly
related to hypertension, with prescription medication alone accounting for onehalf
of the expenditure. Health preactitioners following established treatment
protocols is important in helping control the costs of hypertension, as deviations
from established protocols are estimated to cost an additional 13 billion USD
annually. Almost 10% of this cost is caused by patients being given inappropriate
prescriptions that are inconsistent with evidenced-based recommendations.
Global financial burden of hypertension
The total cost of hypertension has also been studied globally. These studies have
taken into account costs associated with both hypertension and prehypertension.
The International Society of Hypertension tried to quantify the cost of treating
elevated BP and diseases related to elevated BP (including new cases of ischemic
heart disease and stroke) and estimated that 370 billion USD was spent around the
world in 2001 because of non-optimal BP levels. This global estimate suggests that
the direct cost of non-optimal BP control accounts for about 10% of all healthcare
expenditure. To put this into perspective, because the World Bank defines the
world’s poorest citizens as those living below 1 USD/day, a 370 billion USD
expenditure could raise all of these one billion citizens out of extreme poverty,
highlighting both the magnitude of the expense and the benefits that could be
realized if hypertension could be eliminated.
Other costs of hypertension
There are also ‘indirect costs’ of hypertension, including loss of life and loss of
productivity due to absenteeism, illness, and death. Globally, it has been estimated
that hypertension accounts for 14% of deaths, and approximately 6% of disabilityadjusted
life years (a measure of work time lost to disability) can be attributed
to non-optimal BP. Although such indirect costs are obviously substantial, their
precise financial burden is difficult to estimate.
Total costs of hypertension
The total cost of hypertension, using direct costs (treatment of hypertension
and related medical conditions) and indirect costs (loss of productivity and
life), is estimated at a staggering four trillion USD globally. It is obvious that
hypertension – both controlled and uncontrolled – is a costly and likely unstainable
burden demanding much more attention than it currently receives.






